UNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
_________________________
FORM 10-K
_______________________________
(Mark One)
| | | | | |
| ☒ | ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the year ended December 31, 2025
OR
| | | | | |
| ☐ | TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934 |
For the transition period from to
Commission file number 001-40365
_________________________
Privia Health Group, Inc.
(Exact Name of Registrant as Specified in Its Charter)
_________________________
| | | | | | | | | | | |
Delaware | | 81-3599420 |
(State or other jurisdiction of incorporation or organization) | | (I.R.S. Employer Identification No.) |
| | | |
| 950 N. Glebe Rd., | | |
| Suite 700 | | |
| Arlington, | Virginia | | 22203 |
(Address of Principal Executive Offices) | | (Zip Code) |
(571) 366-8850
(Registrant's telephone number, including area code)
Securities registered pursuant to Section 12(b) of the Act: | | | | | | | | |
| Title of each class | Trading Symbol(s) | Name of each exchange on which registered |
| Common Stock, $0.01 par value per share | PRVA | The Nasdaq Global Select Market |
Securities Registered Pursuant to Section 12(g) of the Act: None
Indicate by check mark if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. Yes ☒ No ☐
Indicate by check mark if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. Yes ☐ No ☒
Indicate by check mark whether the registrant: (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. Yes ☒ No ☐
Indicate by check mark whether the registrant has submitted electronically every Interactive Data File required to be submitted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit such files). Yes ☒ No ☐
Indicate by check mark whether the registrant is a large accelerated filer, an accelerated filer, a non-accelerated filer, a smaller reporting company, or an emerging growth company. See the definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company,” and “emerging growth company” in Rule 12b-2 of the Exchange Act.
| | | | | | | | | | | |
| Large accelerated filer | ☒ | Accelerated filer | ¨ |
| Non-accelerated filer | ¨ | Smaller reporting company | ☐ |
| | Emerging growth company | ¨ |
If an emerging growth company, indicate by check mark if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. ☐
Indicate by check mark whether the registrant has filed a report on and attestation to its management’s assessment of the effectiveness of its internal control over financial reporting under Section 404(b) of the Sarbanes-Oxley Act (15 U.S.C. 7262(b)) by the registered public accounting firm that prepared or issued its audit report. ☒
If securities are registered pursuant to Section 12(b) of the Act, indicate by check mark whether the financial statements
of the registrant included in the filing reflect the correction of an error to previously issued financial statements. ☐
Indicate by check mark whether any of those error corrections are restatements that required a recovery analysis of incentive-based compensation received by any of the registrant’s executive officers during the relevant recovery period pursuant
to §240.10D-1(b). ☐
Indicate by check mark whether the registrant is a shell company (as defined in Rule 12b-2 of the Act). ☐ No ☒
As of February 20, 2026 the registrant had outstanding 123,688,289 shares of common stock, $0.01 par value. As of June 30, 2025 (the last business day of the registrant’s most recently completed second fiscal quarter), the aggregate market value of the common stock held by non-affiliates was approximately $1.75 billion based on the closing price per share of common stock on that date of $23.00 as reported on the Nasdaq.
DOCUMENTS INCORPORATED BY REFERENCE
Portions of the information called for by Part III of this Annual Report on Form 10-K is hereby incorporated by reference from the proxy statement for the registrant’s 2026 annual meeting of stockholders, which proxy statement will be filed with the Securities and Exchange Commission no later than 120 days after the registrant’s fiscal year ended December 31, 2025.
TABLE OF CONTENTS
INFORMATION REGARDING FORWARD-LOOKING STATEMENTS
This Annual Report on Form 10-K contains forward-looking statements. We intend such forward-looking statements to be covered by the safe harbor provisions for forward-looking statements contained in Section 27A of the Securities Act of 1933, as amended (the “Securities Act”), and Section 21E of the Securities Exchange Act of 1934, as amended (the “Exchange Act”). In some cases, you can identify these statements by forward-looking words such as “may,” “might,” “will,” “should,” “expects,” “plans,” “anticipates,” “believes,” “estimates,” “predicts,” “potential” or “continue,” the negative of these terms and other comparable terminology. These forward-looking statements, which are subject to risks, uncertainties and assumptions about us, may include projections of our future financial performance, our anticipated growth strategies and anticipated trends in our business. These statements are only predictions based on our current expectations and projections about future events. There are important factors that could cause our actual results, level of activity, performance or achievements to differ materially from the results, level of activity, performance or achievements expressed or implied by the forward-looking statements. These risks and uncertainties include factors related to, among other things:
•the heavily regulated industry in which we operate, and any failure by us to comply with applicable healthcare laws and government regulations, which could result in our incurring financial penalties and becoming excluded from participating in government health care programs;
•the impact of changes in applicable laws, rules or regulations, including with respect to health plans and payers and our relationships with such plans and payers, and provisions that impact Medicare and Medicaid programs;
•our dependence on relationships with Medical Groups (defined herein), some of which we do not own;
•our growth strategy, which may not prove viable and we may not realize expected results;
•difficulties implementing our proprietary end-to-end, cloud-based technology solution (the “Privia Technology Solution”) for Privia Physicians (defined herein) and new Medical Groups;
•the high level of competition in our industry and any failure by us to compete effectively and innovate;
•challenges in successfully establishing a presence in new geographic markets, acquiring entities or assets, or integrating new markets;
•our reliance on our electronic medical record (“EMR”) vendor, athenahealth, Inc., which the Privia Technology Solution is integrated and built upon;
•changes in the payer mix of patients and potential decreases in our reimbursement rates from commercial payers, including as a result of consolidation in the industry;
•the financial and operational impact of our compliance with various complex and changing federal and state privacy and security laws and regulations related to our use, disclosure, and other processing of personal information and protected health information, including the Health Insurance Portability and Accountability Act of 1996, as amended from time to time (collectively, “HIPAA”);
•the impact of actual and potential cybersecurity incidents or privacy or security breaches involving us, our vendors or other third parties;
•the continued availability of a qualified workforce, including staff at our Medical Groups, and the continued upward pressure on compensation for such workforce; and
•other risk factors described in our Annual Report on Form 10-K for the year ended December 31, 2025 (the “Annual Report”) and other filings with the Securities and Exchange Commission (“SEC”).
You should read this Annual Report and the documents that we reference in this Annual Report and have filed as exhibits to this Annual Report with the understanding that our actual future results, levels of activity, performance and achievements may be materially different from what we expect. We qualify all of our forward-looking statements by these cautionary statements. These forward-looking statements speak only as of the date of this Annual Report. Except as required by applicable law, we do not plan to publicly update or revise any forward-looking statements contained in this Annual Report, whether as a result of any new information, future events or otherwise.
PART I
ITEM 1. BUSINESS
Overview
Privia Health Group, Inc. (“Privia Health”, “we”, “our”, or the “Company”) is a technology-driven, national physician-enablement company that collaborates with physician practices, health plans, and health systems to achieve the quadruple aim of better outcomes, lower costs, improved patient experience, and happier and more engaged providers. We seek to accomplish the quadruple aim by entering markets and organizing existing physicians and non-physician clinicians into a unique practice model that combines the advantages of a partnership in a large regional medical group (each, a “Medical Group”) with significant provider autonomy for the physicians (collectively, “Privia Physicians”) and non-physician clinicians (collectively “Privia Clinicians” and, together with the Privia Physicians, the “Privia Providers”) in our Medical Groups.
We organize physicians into cost efficient, value-based and primary-care centric networks bolstered by strong physician governance, and promote a culture of physician leadership. Our technology and service solutions (collectively, the “Privia Platform”) are powered by our Privia Technology Solution that integrates both Privia-developed and third-party applications into a seamless interface and workflow that manages all aspects of our Privia Providers’ provision of healthcare services. We enhance the patient experience, improve practice economics and influence point of care delivery through investments in data analytics, revenue cycle management (“RCM”), practice and clinical operations and payer alignment. The Privia Platform is designed to succeed across demographic cohorts, acuity levels and reimbursement models, including traditional fee-for-service Medicare, the Medicare Shared Savings Program (“MSSP”), Medicare Advantage, Medicaid, commercial insurance and other existing and emerging direct contracting programs with payers and employers.
We designed the Privia Platform to be scalable, allowing us to grow our presence in new geographic markets and guide those markets from fee-for-service (“FFS”) to value-based care (“VBC”), including commercial risk, by shifting the reimbursement model and helping our Privia Providers better manage the cost of care through a focus on quality and success-based reimbursement. Our business model is designed to have meaningful revenue visibility, with low invested capital and attractive margin opportunity. We believe the Privia Platform aligns with the direction healthcare is headed, including (1) a macro shift towards VBC models that focus on delivering coordinated, high quality care at lower total costs, (2) a greater focus on the patient experience and (3) a focus on optimizing provider workflow and bringing back the joy of practicing medicine. Our value proposition and comprehensive solution set address needs across the spectrum of physician practices.
We believe the Privia Platform is differentiated and well positioned to drive sustainable long-term growth because it:
•Addresses a large and growing total addressable market (“TAM”) of providers
•Incorporates a flexible model that is purpose-built to scale nationally by facilitating the entrance into new markets with multiple types of physician practices
•Built on a comprehensive cloud-based technology-enabled platform that is designed to optimize provider workflow across the full continuum of reimbursement environments in virtual and in-person care settings
•Focused on establishing scaled provider groups across each geographical market, resulting in increased relevance with payers and patients
•Designed to transition care delivery in each market from FFS to VBC and to enhance the ability of Privia Providers to manage higher risk patients
•Reduces administrative burden and generally increases provider profitability for community providers
•Led by a team with significant experience leading payer, provider and healthcare information technology organizations
We currently have a presence in 24 states and the District of Columbia, including 9 states in which we only participate in VBC arrangements. Generally speaking, we define a market as a geographic area covered by one of our Medical Groups under a single Tax ID Number (“TIN”). A market could comprise a single state, a part of a state or a group of multiple states and/or districts. We aim to build relationships with key constituents including physicians, non-physician clinicians, patients, government programs, commercial payers and employers. As of December 31, 2025, we had 5,380 Privia Providers who are credentialed and bill for medical services, in both Owned and Non-Owned Medical Groups (as defined below), (“implemented providers”). Our implemented providers operate in over 1,300 practice locations. Privia cares for over 5.8 million patients, including in VBC arrangements approximately 910,000 commercial patients, as measured at the end of a particular period (“attributed lives”), approximately 212,000 Medicare Advantage attributed lives, 298,000 Medicare Shared Savings / Maryland PCP+ Program attributed lives, and approximately 120,000 Medicaid attributed lives. In some instances, we also move into and expand in new and existing markets through our Privia Care Partners model, which offers an affiliation model to providers who are looking solely for VBC solutions. For those practices, we furnish population health services, reporting and analytics, along with certain management services.
Under our Privia Medical Group model, Privia Physicians join the Medical Group in their geographic market as an owner of the Medical Group. We own a majority interest in certain of our Medical Groups (each, an “Owned Medical Group”), with Privia Physicians collectively owning a minority interest, and we own no interest in certain other Medical Groups for which we provide services through a services agreement (each, a “Non-Owned Medical Group”). In those markets in which state regulations prohibit us from owning Medical Groups, the Non-Owned Medical Groups may be owned by the Privia Physicians or majority owned indirectly by a licensed physician holding a Privia leadership position (each such Non-Owned Medical Group owned in this manner, a “Friendly Medical Group”) with Privia Physicians collectively owning a minority interest. In certain markets where we partner with health systems, our health system partner owns a majority interest in the Non-Owned Medical Groups, with Privia Physicians owning a minority interest. Privia Physicians furnish healthcare services through our Medical Groups and continue to own their historical practice entities (“Affiliated Practices”), which provide certain services to the Medical Groups, such as use of space, non-physician staffing, equipment and supplies.
We provide management services to the Medical Groups though local management services organizations (each, an “MSO”), which provide Medical Groups with access to VBC opportunities either directly or through Privia-owned accountable care organizations (each, an “ACO”). We have national committees that distribute quality guidance, and we employ Chief Medical Officers who provide clinical oversight and direction over the clinical affairs of the Owned Medical Groups. Additionally, we hold the provider contracts, maintain the patient records, set reimbursement rates, and negotiate payer contracts on behalf of the Owned Medical Groups.
We principally derive our revenues from the following four sources: (i) FFS-patient care revenue generated from providing healthcare services to patients through Privia Providers of Owned Medical Groups and Friendly Medical Groups, in addition to management and administrative services earned for administrative services provided to Non-Owned Medical Groups (“FFS-administrative services”), (ii) per member per month (“PMPM”) care management fees, including management and administrative fees, (iii) VBC revenue collected on behalf of our Privia Providers in the form of (a) capitated revenue and shared savings, including quality performance-based bonuses, and (iv) other revenue from additional services offered to Privia Providers or directly to patients or employers, such as concierge services, virtual visits, virtual scribes and coding, clinical trials, behavioral health management, and partnerships with self-insured employers to offer direct primary care to their employees. The operations of our Owned Medical Groups, owned ACOs, owned MSOs and Friendly Medical Groups are reflected within our consolidated financial results.
We seek to reimagine the approach to managing physician organizations and optimize their performance by (i) focusing on technology and population health, (ii) establishing a single-TIN Medical Group and governance model in each geographic market, (iii) owning and operating an MSO in each local market, (iv) building or acquiring ACOs to capture VBC opportunities, and (v) offering a high quality, low cost provider network for purchasers and payers.
Trends impacting the U.S. healthcare system
Challenges Physicians Confront Today
Physicians across the country face tremendous challenges in managing their practices. Physician practices have seen declines in profitability, limited access to capital and strained cash flows as the administrative burden to manage patients has increased. Complexity in payment models, including changes in reimbursement, and outdated technology has also led to physician burn-out and has hindered physician to patient interactions. Healthcare insurance companies have narrowed their networks, leading to volume pressures that particularly impact independent practitioners. Physicians are at the center of these issues and are the key to the solution.
Rising Healthcare Costs
Health expenditures in the United States grew 7.2% to reach $5.3 trillion in 2024, or $15,474 per person, according to Centers for Medicare and Medicaid Services (“CMS”), representing approximately 18.0% of U.S. GDP. National health expenditures are projected to reach $8.6 trillion or 20.3% of GDP by 2033, according to CMS, outpacing average GDP growth.
Transition to VBC
Historically, healthcare delivery has centered on reactive care to acute events, which resulted in the development of an FFS payment model. By linking payments to volume of encounters and pricing for higher complexity interventions, the FFS model does not reward prevention, but rather unintentionally incentivizes the treatment of acute care episodes as they occur. With our experience working in all reimbursement environments and expertise in VBC and assisting providers in the transition to VBC, Privia enables providers to accelerate and navigate this transition.
We accelerate our go-to-market strategy using on the ground market intelligence and a data driven approach to add new practices to our Medical Groups. As our Medical Groups grow, we transition our markets to VBC programs as demonstrated by the increase in our attributed risk lives across various programs.
Our Market Opportunity
Our growth strategy is centered on capturing opportunities in existing markets and entering multiple new markets nationally over the next decade.
According to Statista, there were approximately 1,000,000 total physicians and providers in the U.S. as of May 2024. Nephron Research estimated in a December 2024 research report titled “Healthcare Services 2025 Outlook” that the “physician enablement” market in which we participate represents up to $2.4 trillion of that total healthcare spend. We believe the flexibility of our model uniquely positions us to address this large market opportunity.
We understand that healthcare is local and that providers have insight into the needs of their patients and their community. With these issues in mind, Privia has been purpose-built to address a large market opportunity. Unlike industry players who focus only on point solutions or narrow patient cohorts, we offer a national platform with localized solutions designed to meet the needs of physicians, patients and payers. We offer these dedicated providers the benefits of a larger organization while maintaining significant provider autonomy.
Privia collaborates with an anchor medical group or a health system that has strong physician leadership and interest in embracing and amplifying VBC in its local market. We then develop a network around primary care providers and specialists.
Our goal since inception has been to solve problems physicians face regardless of reimbursement environment or patient type. As such, we deploy our solution across the healthcare continuum. Our model is designed for all provider specialties and reimbursement environments and with all payer types.
The Privia Platform and Business Model
Single-TIN Medical Group: Generally, we establish a primary care centric single-TIN Medical Group in our markets that facilitates payer negotiation, clinical integration and alignment of financial incentives. Our Medical Group governance structure allows Privia Providers to build a clinical culture that adapts to consumers’ and a region’s unique and evolving needs. Privia Providers in our Medical Groups collaborate in physician-organized delivery meetings to review performance data, share best practices, create an environment of accountability, and advance evidence-based medicine while maintaining significant provider autonomy. At the local leadership level, Privia Physicians across different practice locations meet regularly with support from Privia performance team members to drive local population health initiatives, engagement and performance. At the market Medical Group level, Privia Physicians, along with Privia team members, advise on priorities, set annual objectives, and approve payer contracts and performance distribution. Finally, at the national level, our Privia Physicians receive input from each market and establish priorities for operational improvements and clinical priorities. We believe that this integrated governance structure allows our Privia Physicians to focus on taking care of patients. The structure also allows Privia Providers to share ideas in a broader forum, sharing best practices with each other.
Management Services Organization: Our market-level MSOs leverage our scale to reduce administrative work, increase efficiency, and lower direct costs for our Privia Providers. Our payer contracting team works with multiple private and government payers across markets to construct and participate in VBC programs. Our team of performance consultants conduct business operations reviews and provide advice on optimizing our Privia Physicians’ finances and productivity. Our procurement team develops opportunities to reduce provider expenses through participation in group purchasing. Our analytics team enables our Privia Providers to make more data-driven decisions on financial, operational, and clinical initiatives, resulting in same store practice growth across both FFS and VBC programs. Our clinical operations and informatics team works to include the “doctor’s voice” in our technology solutions to drive savings and optimize patient outcomes. Our innovative technology improves data security, bolsters the patient-provider relationship, and offers patients a seamless, coordinated experience.
Accountable Care Organizations: Our physician-led, local market-based ACOs aim to lower costs, engage patients, reduce inappropriate utilization, and improve coordination and patient quality metrics to drive VBC. Our scale and quality metrics allow us to enhance reimbursements for delivering high-quality care. The Privia Platform identifies quality gaps, sends patient satisfaction surveys, automates patient outreach and education, and generates reports and alerts to improve care coordination. Our platform proactively shares critical information at various points along the continuum of care to advance population health and streamline provider workflow. Our integrated tools result in cost savings for Privia Providers in both commercial and federal programs by diverting costly patient encounters.
In 2024, Privia operated nine ACOs that delivered care to more than 194,000 Medicare beneficiaries through MSSP, achieving shared savings of $233.1 million, an increase of 32% over 2023. Our per capita expenditures per member per year were 8% lower than the median MSSP ACO and 22% lower than total FFS Medicare. On a per capita or rate of use basis, our weighted average realized emergency department visits was 17% lower than the median MSSP ACO and 25% lower than total FFS Medicare; our weighted average outpatient facility spend was 23% lower than the median MSSP ACO and 35% lower than total FFS Medicare; and our weighted average inpatient facility spend was 13% lower than the median MSSP ACO and 28% lower than total FFS Medicare. Since 2014, we have delivered total shared savings across government programs and commercial payers of more than $1.5 billion, including $922 million through participation in the MSSP. Our approach has been successful across Commercial, Medicare Advantage, MSSP, and Medicaid, from simpler pay-for-performance programs to more complex partial capitation and risk-based programs.
For the 2025 MSSP performance year, Privia had a total of ten ACOs serving over 298,000 Medicare beneficiaries. Out of the ten ACOs, six were participating in the MSSP Enhanced Track with potential upside and downside financial risk.
Network for Purchasers and Payers: Our Medical Groups enable providers to connect across our platform to better understand the holistic needs of each patient and connect them with other providers to address their individual medical needs. This is accomplished by leveraging data from numerous sources and utilizing provider input based on local knowledge to develop aligned virtual preferred networks that are designed to address the unique needs of government and commercial payers as well as individual employers. We build these networks within our platform to enhance both the provider and the patient experience by removing administrative burden and enhancing efficient and coordinated patient communication. This capability also allows us to work with health systems to increase alignment with employed, affiliated and independent physicians to optimize resource utilization through our model.
Payers: We align incentives with our payer partners by linking performance to rewards and enter into custom contracts serving all demographics and populations across the continuum of care.
Employers: We work with employers to deliver customized medical benefits packages supported by our provider networks. Our enhanced primary care model offers quality care to their employees while lowering per-member, per-year costs. Our networks connect primary care and specialty providers to coordinate and streamline employee care.
The Privia Technology Solution: Our End-to-End Technology-Enabled Platform
The Privia Technology Solution streamlines the provider, patient and care team workflows focusing on each of the following aspects: (i) patient access through various avenues (patient portal, mobile app and search engine optimization), (ii) pre-visit analytics and preparation, (iii) in-person or virtual care delivery and (iv) post visit analytics, care-coordination and reporting. The Privia Technology Solution enables us to scale operations in multiple markets, enhance performance across multiple payer contracts and deliver superior quality care to patients across the demographic spectrum.
The Privia Technology Solution supports providers, including by leveraging machine learning and artificial intelligence (“AI”) to reduce or automate certain administrative tasks. In addition, the Privia Technology Solution helps us scale operationally, as our product designers and engineers collaborate closely with clinical and operational teams to optimize workflows as we enter new markets and new payer contracts. The Privia Technology Solution is built on a modern cloud-based technology stack employing agile development cycles. Our technology architecture utilizes API standards for ease of implementing new functionalities and integrating with multiple external systems.
Patient Access: We optimize practices’ web presence so patients can find and schedule an appointment with a provider online and receive appointment reminders. We offer a mobile app and patient portal that allow patients to access personal health information and stay connected with their providers by equipping physicians with the tools they need to deliver quality, affordable care when, where, and how patients need it. We also provide 24/7 Nurse Triage Call Center and 24/7 On-demand Virtual Visits for immediate or primary care.
Pre-visit: Our technology and tools embed insights directly into our EMR so providers can assess both patients’ health and practice performance. We acquire data from across the healthcare ecosystem for a single view of the patient. Privia’s solutions identify opportunities before the patient visit, using huddle reports and patient stratification. The Privia Platform allows providers to identify patient attribution, open quality gaps, open coding gaps, assess patient risk level and determine care management eligibility.
During Visit: The Privia Technology Solution integrates workflows designed to allow providers and care teams to close quality gaps, prioritizes key risk adjustment gaps, recaptures prior diagnoses and embeds suspect medical conditions within the EMR.
Between Visits: We also provide patient education tools, automated standing orders based health event data triggers, transitional and chronic care management, and care plans. We use patient-satisfaction feedback to increase practices’ online visibility. Our system sends secure messages to patients within the patient portal and messages are sent on behalf of the provider and care team. Our proprietary care team application is integrated within the EMR and patient portal enabling clinical assessments and templates to guide care team’s workflows. We also provide a resource hub and training platform for Privia Providers.
Virtual Visit Capabilities
Our virtual health capabilities are fully integrated with our patients’ EMR so our primary care providers can readily access data from virtual visits. Our patients can also use the telehealth platform to schedule a virtual visit with a provider of their choice, an in-person follow-up visit or a referral to a specialist.
As of December 31, 2025, over 1.5 million distinct Privia Health patients have completed over 4.7 million virtual visits. Of all patients seen by a Privia Provider virtually, over 95% did not return to the same doctor or another doctor in the same specialty for a follow-up visit within seven days.
Governance and Physician Leadership Culture
Our multipurpose governance model includes a local governance structure tailored to each market that is intended to improve aspects of our patient, physician and payer relationships. Privia Physicians hold the majority of board positions in our Owned Medical Groups and ACOs, including authority over matters related to the practice of medicine, and we either have exclusive authority over certain strategic issues such as mergers and acquisitions, and termination of our MSA or veto authority relative to certain strategic decision making. In addition, our National Physician Advisory Council (“NPAC”) brings together the clinical and executive local market
leadership across the country to provide valuable input to improve the Privia Platform, physician facing data reporting, common quality initiatives, marketing and product performance.
Under the auspices of the NPAC, various individual specialty collaboratives meet both locally and nationally to address common issues, bring best practices and models of success to the forefront. As an example, Privia Women’s Health focuses on advancing VBC and performance in women’s health, including participation in building VBC-contracting models with bundled payments and episodes of care, and including remote patient monitoring in pregnancy. The pediatric collaborative brings forward strategies to engage patients and families in continuing pediatric care through continuous education, information, structural changes and other ways of keeping patients and family safe including virtual visits, vaccination programs, and triaging for in person visits.
Our Growth Strategy
Our growth strategy is centered on capturing opportunity in existing markets and entering new markets through the following strategies:
Organic Growth in Existing Practices
•Patient panel and volume growth through enhanced patient experience and value-based clinical model, which increases retention and drives new patient referrals;
•New provider growth through strategic expansion, succession planning, and use of advanced practice practitioners;
•Expansion of practice services such as more convenient virtual care and in-office ancillaries; and
•Revenue optimization through enhanced payer contracting strategies and strong revenue cycle performance which drives efficiency and higher revenue realization.
Moving Markets to VBC
•Focus on same store growth of patients attributed to value-based contracts in each existing geographic market;
•Increase our revenue opportunity on a per patient basis by continuing to improve performance and financial value in existing and new value-based programs across commercial, MSSP, Medicare Advantage, Medicaid and other existing and emerging direct payer and employer contracting programs; and
•Develop new products and programs in partnership with aligned payers that are built with and around our network of physicians and providers.
White Space Opportunities in Existing Markets
•We intend to add primary care and specialist practices in existing markets to enhance growth. Our data-driven approach allows us to identify primary care and specialist provider groups that we believe may benefit from our platform;
•Expand Privia Women’s Health and Privia Pediatrics platforms;
•Develop value-oriented ancillary services for our Medical Groups. This includes leveraging existing platforms of providers and patients to provide ancillary services (e.g., clinical laboratory, imaging and pharmacy) within our Medical Groups;
•Expand relationships with self-insured employers, businesses, schools, universities, and third-party administrators seeking population health and virtual care solutions;
•Continue to pursue direct contracting opportunities, including direct primary care and onsite / near-site clinics fully integrated with our local Privia networks; and
•Expand our clinical research program by designing and executing on clinical trials across multiple therapeutic areas.
New Market Development
•Our data-driven market selection process identifies expansion opportunities and informs our approach to opening new geographies; and
•We evaluate the broader market landscape for opportunities on a continuous basis and proactively develop relationships before committing to enter a market.
Disciplined and Strategic Acquisitions and Investments
•Our growth playbook also factors in the opportunity to acquire minority or majority ownership of provider groups or clinically integrated networks in existing and new markets and we may also open de-novo, wholly or partially owned, sites of care in existing and new markets.
Sales, Marketing and Business Development
We aspire to continue growing our national platform by expanding geographically into new markets and growing within our existing markets. Our business development, sales and marketing initiatives focus on the following avenues to drive growth:
•Anchor health systems and medical groups—We establish customized anchor partnerships with leading medical groups and health systems in new markets developed from long-term relationships led by our business development team. We use a data driven approach to qualify, segment, and evaluate new market opportunities. We collaborate with leading medical groups and health systems looking to capitalize on the opportunity to create next generation physician led medical groups and transition their local markets to VBC.
•Existing market provider growth—Our in-market and national sales and marketing teams work together to add new medical groups, physician practices and individual providers in existing markets. We accelerate our go-to-market strategy using on the ground market intelligence and a data driven approach. Our enterprise sales force is comprised of an in-house group of sales professionals organized by market. Our sales operations team supports our sales force with lead generation, while our growth analytics team conducts financial and operational analysis on our value proposition for prospective partners. Our provider recruitment team assists our existing practices in hiring new providers, from sourcing through onboarding.
•Consumer sales and marketing—As our medical groups grow in each market, we look to transition the market to value-based programs by increasing the patient panels of our providers and adding attributed risk lives across various VBC programs. Our marketing and communications team operates our brand management, enterprise web presence and certain practice location websites, and creates other forms of patient communication and engagement materials. Our branding and marketing strategy to drive growth to our practices have continued to result in increased engagement with new and existing patients and expanded enterprise web presence.
Our marketing strategy focuses on increasing the overall brand awareness of Privia Health and of our Medical Group brands in each of our markets. We run targeted advertisements through print, direct mail, Google search, and social media for provider and patient acquisition. We also develop thought leadership content such as white papers, e-brochures, and blog posts and use public relations to secure earned media placements. Additionally, we participate in industry conferences, and collaborate with media outlets, industry associations, event venues, and local businesses to increase brand awareness. In each of our markets, local independent doctors unite together to form the larger Privia Medical Group. The local practice locations maintain their legacy brand, but also adopt the overarching Privia Medical Group brand.
Competitive Landscape
We compete in a highly fragmented and competitive U.S. healthcare industry. We face competition in each geographic market from a variety of community-based healthcare provider organizations, including large physician practices, independent physician associations, hospitals and health systems, physician-hospital organizations as well as emerging companies, vertically integrated healthcare companies, and private equity firms acquiring and rolling up specialty physician practices. In addition, nationally, we face competition for talent, resources, physicians, and payer contracts from existing and emerging companies in the physician enablement industry segment. We believe our practice model and breadth of services offered to all patient types is unique, and we therefore compete with different companies across certain lines of business, including companies with: dedicated brick-and-mortar locations which often target patients covered by Medicare Advantage plans; dedicated, direct primary care locations which often target a commercial or employer-based patient population; the ability to organize providers into accountable care organizations, allowing physicians to participate in VBC arrangements; and the ability to partner with physicians groups to enable better care delivery primarily for seniors. These competitors may be narrower in their competitive footprint and may not address all the key stakeholders we serve simultaneously. Our indirect competitors also include episodic point solutions, such as telemedicine offerings, as well as urgent care providers. Our competitive success is contingent on our ability to address the needs of our key stakeholders efficiently and cost effectively compared with competitors. We expect to face increasing competition, both from current competitors, who may be well established and enjoy greater resources or other strategic advantages to compete for some or all key stakeholders in our markets, as well as new entrants into our market.
Given the size of the healthcare industry, we expect additional competition, including potentially from new companies, smaller emerging companies which could introduce new solutions and services, as well as other incumbent players in the healthcare industry, private equity firms or from broader industry players who could develop their own offerings and may have substantial resources and relationships to leverage. With the emergence of new technologies and market entrants, we expect to face increasing competition over time, which we believe will generally increase awareness of the need for modernized care models and other innovative solutions.
Intellectual Property
We rely on a combination of trademarks, service marks, copyrights and trade secrets to protect our proprietary technology and other intellectual property. As of December 31, 2025, we exclusively own six (6) registered trademarks in the United States, including Privia Health. In addition, we have registered domain names for websites that we use or may use in our business.
We seek to control access to and distribution of our proprietary information, including our algorithms, source and object code, designs, and business processes, through security measures and contractual restrictions. We seek to limit access to our confidential and proprietary information to a “need to know” basis and enter into confidentiality and nondisclosure agreements with our employees, consultants, customers and vendors that may receive or otherwise have access to any confidential or proprietary information. We also obtain written invention assignment agreements from our employees, consultants, and vendors that assign to us all right, interest, and title to inventions and work product developed during their employment or service engagement with us. In the normal course of business, we provide our intellectual property to external parties through licensing or restricted use agreements. We have established a system of security measures to help protect our computer systems from security breaches and computer viruses. We have employed various technology and process-based methods, such as clustered and multi-layer firewalls, intrusion detection systems, vulnerability assessments, threat intelligence, content filtering, endpoint security (including anti-malware and detection response capabilities), email security mechanisms, and access control mechanisms. We also use encryption techniques for data at rest and in transit. For additional information on risks associated with our intellectual property and information technology systems, see “Risk Factors—Technology, Cybersecurity and Privacy Risks.”
Government Regulations
Our operations, those of our Owned Medical Groups, Non-Owned Medical Groups, and Privia Providers are subject to extensive and complex laws and regulations at the federal, state and local levels relating to, among other issues, billing and coding for, and documentation of, services and properly handling overpayments; relationships with physicians and other referral sources and referral recipients, including, for example, state or attorney general notice or approval requirements for certain relationships; restrictions related to multi-specialty practices; appropriateness and adequacy of medical care; quality of medical equipment and services; patient, workforce, and public safety, as well as patient rights; qualifications and supervision of, and reimbursement for services provided by, medical and support personnel; the provision of services via telehealth, including technological standards and coverage restrictions or other limitations on reimbursement; the confidentiality, maintenance, interoperability, exchange, and security of medical records and other health-related and personal information, including data breach, ransomware and identity theft issues; the development and use of AI and other predictive algorithms, including those used in clinical decision support tools; restrictions on the provision of medical care, including reproductive care; permitting, facility and personnel licensure, certification and accreditation requirements; mandatory reporting requirements for providers; enrollment standards and requirements for participation in government healthcare programs; corporate practice of medicine and fee-splitting; consumer disclosures and price transparency; the distribution, maintenance and dispensing of pharmaceuticals and controlled substances; relationships between healthcare providers and drug and medical device companies; debt collection, balance billing and billing for out of network services; translation services and accessibility requirements; communications with patients and consumers; advertising and marketing; operating policies and procedures; activities regarding competitors; insurance and the assumption of financial risk by healthcare entities, including allowable types of financial risk; addition of facilities and services; and environmental protections.
If any of our operations or those of our Owned Medical Groups, Non-Owned Medical Groups, or Privia Providers fail to comply with these or other applicable laws and regulations, which are subject to change, any such failure could result in liabilities, including civil penalties, money damages, lapses in reimbursement, loss of facility licenses, accreditations, or certifications, revocation of billing privileges, exclusion of one or more entities and/or facilities from participation in the Medicare, Medicaid and other federal and state health care programs, termination of various relationships or contracts, lawsuits and criminal penalties. Medicare and Medicaid payments may be suspended pending even an investigation of what the government determines to be a credible allegation of fraud. We could also be required to make changes to our business model and/or practices, which could increase operating expenses, negatively affect our business relationships, and decrease access to new business opportunities. In addition, different interpretations or enforcement of, or amendments to, these and other laws and regulations in the future could subject current or past practices to allegations of impropriety or illegality or could require us to make changes in our operations, facilities, equipment, personnel, services, capital expenditures and operating expenses. The costs of compliance with, and the other burdens imposed by, these and other laws or regulatory actions may increase operational costs, result in interruptions or delays in the availability of systems and/or result in a decline in patient volume or Privia Provider or Medical Group attrition. Any action against us for violation of these laws or regulations, even if we successfully defend against it, could cause us to incur significant legal expenses, divert our management’s attention from the operation of our business or result in reputational harm.
We expect that our industry will continue to be subject to substantial regulation, the scope and effect of which are difficult to predict. Our activities could be subject to investigations, audits and inquiries by various government and regulatory agencies and commercial payers with whom we contract at any time in the future. Adverse findings from such investigations and audits could bring severe consequences that could have a material adverse effect on our business, results of operations, financial condition, cash flows, reputation and stock price. In addition, commercial payers could require pre-payment audits of claims, which can negatively affect cash flow, or terminate contracts, including for repeated deficiencies.
Furthermore, if a state in which we currently operate, or in which we seek to expand, views the participation of the Company or its Medical Groups in risk-sharing arrangements as the assumption of insurance risk, the arrangement may fall within the purview of state insurance or managed care laws and regulations, and we or the Medical Group may be required to obtain a state insurance or managed care license or similar registration. These laws and regulations may subject the entity involved to oversight by state regulators, including through periodic reporting or audits, and requirements for financial reserves. Some of these laws may be vague and state regulators may have interpretations that differ from ours. Even if a state regulatory agency does not directly oversee the transfer of risk by a payer to a downstream entity, the state may require the licensed payer to include certain oversight mechanisms in payer contracts, which could increase our or our Medical Groups’ administrative costs and have an adverse effect on our business, cash flows or results of operations. If we or our Medical Groups fail to comply with insurance laws and regulations, including licensure and oversight requirements, we may be required to make changes to our operations and could be subject to civil and/or criminal penalties, denial of future licensure applications and termination of payer contracts. These laws and regulations may affect the operation of, for example, ACOs, direct primary care programs, provider-sponsored organizations, independent practice associations, clinically integrated networks, and provider capitation models. At the state level, our ability to conduct business and the structure of our operations depends on each state’s laws, regulations, and policies governing, among other issues, the corporate practice of medicine, fee-splitting, and the assumption of financial risk.
Corporate Practice and Fee-Splitting Laws
At the state level, our ability to conduct business and the structure of our operations depends on each state’s laws, regulations, and policies governing, among other issues, the corporate practice of medicine, fee-splitting, and the assumption of financial risk. In several states, laws and regulations, guidance from professional licensing boards or state attorneys general and judicial doctrines prohibit corporations and other entities not owned by physicians or other permitted health professionals from practicing medicine and other professions. These laws and doctrines have been interpreted in some states to prohibit entities not owned by permitted professionals from employing physicians and other professionals and to prohibit such entities from undertaking activities that could be seen as exercising control over healthcare provider professional judgment. Some states also have adopted restrictions on direct or indirect payments to, or entering into fee-splitting arrangements with, physicians and unlicensed persons or business entities. These restrictions vary by state and are often vague and subject to interpretation by state medical boards, state attorneys general and other regulatory authorities. We attempt to structure our arrangements with healthcare providers to comply with applicable state law. However, we cannot provide assurance that governmental officials responsible for enforcing these laws will not assert that we, or transactions in which we are involved, violate these laws. These laws may also be interpreted by courts in a manner inconsistent with our interpretations. Possible sanctions for violations of these restrictions include loss of a physician’s license and civil and criminal penalties. In addition, agreements between the Company and physicians may be considered void and unenforceable, our MSAs and management fees could be adversely affected, and we may be required to restructure the Company’s relationships with Medical Groups and Privia Providers, any of which could have a material adverse effect on our business, financial condition and results of operations.
Federal Anti-Kickback Statute, Stark Law and Similar State and Federal Laws
Some healthcare laws apply to the financial relationships we have or our Medical Groups have with physicians and others who either refer or influence the referral of patients to our Medical Groups and Privia Providers or who are the recipients of referrals. The federal Anti-Kickback Statute, for example, is a criminal law that prohibits, among other things, the solicitation, receipt, offering or payment of any remuneration with the intent of generating referrals or orders for services or items that may be paid for by a federal healthcare program. The Office of the Inspector General for the U.S. Department of Health and Human Services (“OIG”) has enacted safe harbor regulations that outline practices deemed protected from prosecution under the federal Anti-Kickback Statute. In addition to the Anti-Kickback Statute, in October 2018, the U.S. enacted the Eliminating Kickbacks in Recovery Act of 2018 (“EKRA”), as part of the Substance Use-Disorder Prevention that Promotes Opioid Recovery and Treatment for Patients and Communities Act. EKRA is an all-payer anti-kickback law that makes it a criminal offense to pay any remuneration to induce referrals to, or in exchange for, patients using the services of a recovery home, a substance use clinical treatment facility, or laboratory. While EKRA may have been intended to address inducements related to substance use recovery and treatment, the language in EKRA is broadly written. No regulations have yet been issued clarifying EKRA’s scope and intent. While we and our Medical Groups endeavor to comply with applicable safe harbors, certain current arrangements, including joint ventures and financial relationships with physicians and other referral sources and persons and entities to which our Medical Groups refer patients, may not qualify for safe harbor protection. Failure to qualify for a safe harbor does not mean the arrangement necessarily violates the federal Anti-Kickback Statute, but may subject the arrangement to greater scrutiny. Allegations of violations of the federal Anti-Kickback Statute may also be brought under the federal Civil Monetary Penalty Law, which requires a lower burden of proof than other fraud and abuse laws. The Stark Law is a strict liability civil law that prohibits physicians from making referrals for “designated health services” payable by Medicare or Medicaid to entities with which the physician or an immediate family member of the physician has a financial relationship, unless an exception applies. The Stark Law further prohibits entities that have received such referrals from filing claims with Medicare (or billing another individual, entity or third party payer) for those referred services. The financial relationships of our Medical Groups with referring physicians and their immediate family members must comply with the Stark Law. We and our Medical Groups attempt to structure those relationships to meet an exception to or otherwise comply with the Stark Law, but the regulations implementing the Stark Law, including the requirements to meet exceptions, are detailed and complex. We do not always have the benefit of significant regulatory or judicial
interpretation of the Stark Law and its implementing regulations. Additionally, violations of the federal Anti-Kickback Statute or Stark Law, improper billing for services to federal healthcare programs, or improper retention of overpayments from federal healthcare programs may be the basis for finding a violation under the federal False Claims Act (the “FCA”), either under a suit brought by the government or by a private person under a qui tam, or “whistleblower,” suit. Many states have also passed anti-kickback statutes and physician self-referral prohibitions similar to the federal Anti-Kickback Statute and the Stark Law. However, in many of the states we operate, these state self-referral prohibitions are often drafted broadly to cover all payers (i.e., not restricted to Medicare and other federal health care programs) or certain programs within the state such as the state Medicaid program or state workers’ compensation program. Generally, however, the exceptions or exemptions under state fraud and abuse laws, are less robust and developed than their federal counter parts. If we, our Medical Groups, Privia Providers or ACO participants fail to comply with these or other applicable laws and regulations, which are subject to change, any such failure could result in significant penalties, adversely impact our business, results of operations, financial condition and/or result in reputational harm.
Data Protection
The data protection landscape is rapidly evolving, and the Company, its Medical Groups, Privia Providers and ACO participants, are and may become subject to numerous state and federal laws, requirements and regulations governing the collection, use, disclosure, retention and security of health-related and other personal information. For example, the HIPAA privacy and security regulations extensively regulate the use and disclosure of personal health information (“PHI”) and require covered entities, including healthcare providers and health plans, and vendors (known as “business associates”) that perform certain services that involve creating, receiving, maintaining or transmitting PHI on behalf of covered entities or other business associates, to implement administrative, physical and technical safeguards to protect the privacy and security of PHI. These laws are complex and subject to change and interpretation, and our approach to compliance with such laws may include reliance on safe harbors or other regulatory rules, including those related to organized healthcare arrangements, which are themselves complex, require resources and investment to manage ongoing compliance, and are subject to change and interpretation, particularly in the current regulatory environment. In addition to HIPAA, there are numerous other laws, regulations, and legislative and regulatory initiatives at the federal and state levels governing the confidentiality, privacy, availability, integrity and security of health-related information and other types of personal information. In many cases, the state laws are more restrictive or impose more obligations than, and may not be preempted by, the HIPAA privacy and security regulations. State laws vary in scope, may apply to employees and business contacts in addition to patients, and may be subject to new and varying interpretations by courts and government agencies, creating complex compliance issues and potentially resulting in exposure to additional expense, adverse publicity and liability. The potential effects of these laws are far-reaching and may require the Company, its Medical Groups, and their third-party service and technology vendors to modify data use, storage, transmission and processing practices and policies, or our approach to compliance with other similar laws, and to incur substantial costs and expenses in order to comply. Failure to comply with these and any other comprehensive privacy laws passed at the state or federal level may result in regulatory enforcement action and reputational harm. We expect that new or modified laws, regulations, regulatory guidance and industry standards concerning privacy, data protection and information security, including those related to specific types of personal data, will continue to be proposed and enacted in various jurisdictions, which could impact our operations and cause us to incur substantial costs.
Healthcare Reform
The healthcare industry has been and continues to be impacted by healthcare reform efforts. For example, the Affordable Care Act affects how healthcare services are covered, delivered and reimbursed and expanded health insurance coverage through a combination of public program expansion and private sector health insurance reforms. Changes in the law’s implementation, subsequent legislation and regulations, state initiatives and other factors, including potential changes to or repeal of the Affordable Care Act as a result of changes in the political landscape, have and may continue to affect the number of individuals that elect to obtain public or private health insurance or the scope of such coverage. Reductions in the number of insured individuals or the scope of insurance coverage may have an adverse effect on our business. In addition, Medicare and Medicaid policies and programs, such as MSSP, are subject to change, and have changed, including as a result of changes in the political landscape. Legislation and administrative actions at the federal level may impact funding for, the structure of, or who may be covered by, the Medicaid or Medicare programs, and may shape administration of the Medicaid program at the state level and Medicare Advantage Programs. Other recent health reform initiatives and proposals at the federal and state levels include those focused on price transparency and out-of-network charges as well as pharmacy and pharmacy benefit manager reform efforts, which may impact prices, the relationships between hospitals, patients, payers, and providers, total cost of care and patient outcomes, and lead to further uncertainty in other participants in the healthcare industry, including employers.
General Corporate Information
Privia Health Group, Inc. (Nasdaq: PRVA) was incorporated in Delaware in 2016. Our website is priviahealth.com.
Our Annual Reports on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K and, if applicable, amendments to those reports filed or furnished pursuant to Section 13(a) of the Securities Exchange Act of 1934, as amended, are available free of charge on or through the Privia Health Investor Relations website at ir.priviahealth.com., as soon as reasonably practicable after we electronically file such material with, or furnish it to, the Securities and Exchange Commission, or the SEC. The SEC’s website, http://www.sec.gov, contains reports, proxy and information statements, and other information regarding issuers that file electronically with the SEC.
The information contained on, or that can be accessed through, our websites is not incorporated by reference into this filing and you should not consider any information contained on, or that can be accessed through, our websites as part of this filing.
We announce material information to the public through a variety of means, including filings with the SEC, press releases, public conference calls, and our website. We use these channels to communicate with investors and the public about our Company, our products and services, and other matters. Therefore, we encourage investors, the media, and others interested in our Company to review the information we make public in these locations, as such information could be deemed to be material information. Information on or that can be accessed through our websites is not part of this Annual Report on Form 10-K, and the website addresses are included as inactive textual references only.
Human Capital Resources
As of December 31, 2025, across Privia Health Group, Inc., we had 1,226 employees in 43 states and the District of Columbia. None of our employees are represented by labor unions or covered by collective bargaining agreements. We consider our relationship with our employees to be good and we have not experienced any work stoppages. We believe our geographically dispersed employees are a competitive advantage. While certain employees work onsite, the majority of our workforce is either remote or a blend of in-office and remote. Our flexible workforce strategy allows us to hire qualified talent irrespective of geographic constraints across many functional roles. Our internal systems and processes are designed to ensure our remote employees are productive, contribute meaningfully, and are able to exceed expectations in their roles.
Talent Development and Engagement
At Privia Health, we value all of our employees and the exceptional talent they bring to our organization, in order to support our physicians, providers, practice location staff, and patients. One of our strategic corporate goals is to grow and develop our workforce, and we have established ongoing leadership development and retention programs intended to support employees in their career progression. This includes an Emerging Leaders Program, a Manager Onboarding program, individual coaching, and ad hoc formal and informal training sessions.
Employee Health and Wellness
Our goal is to comprehensively support our employees, no matter who they are or where they are in life. To further this goal, Privia has introduced nationwide access to virtual mental healthcare as well as comprehensive medical coverage for plan participants. Our Employee Assistance Program (“EAP”) provides support to all employees and their family members who may be experiencing times of crisis. Additionally, we have access to management training on important topics like helping parents return to work or identifying burnout. In addition to these on-demand services, we also offer Mental Health First Aid certification so our managers can recognize and respond to a person experiencing a mental health emergency.
Put People First
Privia Health employees are committed to improving patient care through their support of the physicians, providers, and practice location staff. The Nominating and Corporate Governance Committee assists our Board of Directors (“Board”) in its oversight of talent management, including corporate culture, employee experience, recruiting, retention, attrition, career development and progression, succession, and employee relations.
Privia Health has been honored to be named a Top Workplace for the last three years by Energage locally and nationally both as a large-size company and a healthcare organization. In 2024, we earned additional culture excellence awards from other organizations, highlighting our efforts in employee experience, engagement practices, employee well-being, professional development, purpose and values, leadership, innovation, compensation and benefits, and work-life flexibility.
Serving Our Communities
We encourage and actively support our employees to have a meaningful and positive impact on their communities and contribute to charitable causes by giving their time, talents and resources. The Company supports various charitable organizations throughout the year, focusing our efforts on support for the communities in which Privia Physicians practice. In an effort to provide support to employees in times of a weather event or natural disaster, we have a communication protocol we activate. In advance of an anticipated
weather event, we reach out to all employees and our practices in the area of impact to provide resources and support for appropriate disaster preparation and maintain contact with them throughout the event and until they are fully recovered.
ITEM 1A. RISK FACTORS
RISK FACTORS
Investing in our common stock involves a high degree of risk. You should carefully consider the risks and uncertainties described below, together with all of the other information contained in this report, including our consolidated financial statements and the related notes thereto, before making a decision to invest in our common stock. The risks and uncertainties described below are not the only ones we face. It is not possible to predict or identify all such factors. Additional risks and uncertainties that we are unaware of, or that we currently believe are not material, may also become important factors that affect us. If any of the following risks occur, our business, financial condition, operating results and prospects could be materially and adversely affected. In that event, the price of our common stock could decline, and you could lose all or part of your investment.
Risk Factor Summary
The following is a summary of risk factors that could materially and adversely affect our business, financial condition and results of operations.
•We conduct business in a heavily regulated industry, which increases our costs and could restrict the conduct of our business, and if the Company or our Medical Groups fail to comply with the extensive applicable healthcare laws and government regulations, which may change from time to time, we could suffer adverse financial impacts, be required to make significant changes to our operations, or experience reputational harm, any or all of which may adversely affect our business.
•Our business model relies on a complex legal framework that governs our relationships with Medical Groups and Privia Providers. Legal challenges or shifting interpretations of applicable laws could require us to make significant changes to our operations, which could adversely affect our business.
•Our business, financial condition and results of operations may be adversely affected by changes and uncertainty in the healthcare industry, including health reform initiatives and other changes to laws and regulations.
•We, our Medical Groups and Privia Providers, may be subject to legal proceedings, including litigation, governmental investigations and claims, and payer audits.
•Risks associated with VBC arrangements may negatively impact our business, operations, and financial condition.
•If federal or state healthcare programs or commercial payers reduce reimbursement rates we receive or alter payment terms, if we and our Medical Groups are unable to retain and negotiate favorable contracts with private third-party payers, if insured individuals move to health plans with greater coverage exclusions or restrictions or narrower networks, or if our Medical Groups’ volume of uninsured or underinsured patients increases, or if patient responsibility accounts are not able to be collected, our revenues may decline, adversely affecting our financial condition and results of operations.
•The reimbursement process is complex and may involve delays and other uncertainties, which may adversely affect our business, operations, cash flows, revenues, and earnings.
•The information that we or our Medical Groups provide to Medicare Advantage plans and third-party payers could be inaccurate, incomplete or unsupportable, which could impact result in harm to our business, operations and financial condition.
•Third-party payer controls designed to reduce costs and other payer practices to decrease or review utilization, surgical procedure volumes or reimbursement for services rendered may reduce our revenues.
•If the Company and its Medical Groups are unable to effectively compete, including by innovating and evolving our service offerings, our business, financial condition, and results of operations could be adversely impacted.
•Our sales and implementation cycle can be long and unpredictable and requires considerable time and expense, which may cause our results of operations to fluctuate.
•Our performance depends on our ability to efficiently price the Privia Technology Solution, the Privia Platform, and our Privia operating model and to contract with Medical Groups, Privia Providers, health system partners, ACO participants and third-party payers.
•The success of our business depends on the execution of our growth strategy, which may not prove viable and we may not realize expected results, and if the estimates and assumptions we use to determine the size of our total addressable market, or TAM, are inaccurate, our future growth rate may be impacted and our business could be harmed.
•We may encounter difficulty acquiring entities or assets, face challenges integrating the operations of acquired businesses or realizing expected results or become liable for unknown or contingent liabilities as a result of acquisitions.
•If certain of our vendors do not meet our needs, our business, ability to operate, financial condition, cash flows, results of operations, and relationships with our Medical Groups, Privia Providers and their patients could be negatively impacted.
•If we are not able to maintain and enhance our reputation and brand recognition, including through the maintenance and protection of trademarks, our business and results of operations will be harmed.
•The operations of the Company and its Medical Groups are concentrated in certain U.S. states, which makes us sensitive to regulatory, economic, public health, environmental, competitive and other conditions and changes in these jurisdictions, and we may not be able to successfully establish a presence in new geographic markets.
•Changes in treatment methodologies, trends related to the usage of primary care and specialist healthcare services, or the failure to effectively obtain medical supplies, drugs and other goods for Medical Groups could cause our results of operations to decline.
•Security threats, cybersecurity incidents or other forms of data breaches, catastrophic events and other disruptions to our, our Medical Groups’ and ACOs’, our business partners’ or our vendors’ information technology and related systems could compromise sensitive information related to our business, the Medical Groups or patients, prevent access to critical information, harm patients, require remediation and other corrective action, which can be expensive, and expose us to liability, which could adversely affect our business, operations and reputation.
•If we cannot timely implement the Privia Technology Solution for Privia Physicians and new Medical Groups, or promptly resolve Privia Provider and patient concerns, or if the Privia Technology Solution fails to operate as we expect, our business and results of operations may be adversely impacted, we could be subject to litigation, and our reputation may be harmed.
•If we are unable to obtain, maintain and enforce intellectual property protection for our technology or if the scope of our intellectual property protection is not sufficiently broad, others may be able to develop and commercialize technology substantially similar to ours, and our ability to successfully commercialize our technology may be adversely affected.
•Third parties may allege that we are infringing, misappropriating or otherwise violating their intellectual property rights and in some instances initiate formal legal proceedings, the outcome of which would be uncertain and could have a material adverse effect on our business, financial condition and results of operations.
•If we are unable to protect the confidentiality of our trade secrets, know-how and other proprietary and internally developed information, the value of our technology could be adversely affected.
•Any restrictions on our use of, or ability to license, data, or our failure to license data and integrate third-party technologies, could have a material adverse effect on our business, financial condition and results of operations.
•Our use of “open source” software could adversely affect our ability to offer our services and subject us to possible litigation.
•We face risks associated with healthcare technology initiatives, including those related to sharing patient data and interoperability, as well as our use of certain AI and machine learning models.
•Our use, disclosure, and other processing of personal information, including health-related information, is subject to HIPAA, other federal and state privacy and security regulations, and contractual obligations, and our actual or perceived failure to comply with those regulations or contractual obligations could result in significant liability or reputational harm and, in turn, a material adverse effect on our patient base and revenue.
•We depend on our senior management team and other key employees, and the loss of one or more of these employees or an inability to attract, recruit, motivate, develop and retain other qualified talent, including physicians and non-physician practitioners for our Medical Groups could harm our business, operations and growth strategy.
•Our corporate culture has contributed to our success, and if we cannot maintain this culture as we grow, our business may be harmed.
•We have a history of net losses, we anticipate increasing expenses in the future, and we may not be able to maintain profitability, and our ability to use our net operating losses to offset future taxable income is subject to certain limitations.
•Any limitations imposed by indebtedness or any failure to raise additional capital or generate cash flow to expand our operations could restrict our current and future operations or adversely affect our business and growth prospects.
•We may fail to maintain effective internal control over financial reporting, which may adversely affect investor confidence.
•Our overall business results may suffer from a deterioration of public health conditions associated with a pandemic, epidemic or outbreak of an infectious disease.
Legal and Regulatory Risks
We conduct business in a heavily regulated industry, which increases our costs and could restrict the conduct of our business, and if the Company or our Medical Groups fail to comply with the extensive applicable healthcare laws and government regulations, which may change from time to time, we could suffer adverse financial impacts, be required to make significant changes to our operations, or experience reputational harm, any or all of which may adversely affect our business.
Participants in the healthcare industry are subject to extensive and complex laws and regulations at the federal, state, and local levels relating to, among other issues:
•billing and coding for, and documentation of, services and properly handling overpayments;
•relationships with physicians and other referral sources and referral recipients, including, for example, state or attorney general notice or approval requirements for certain relationships;
•restrictions related to multi-specialty practices;
•appropriateness and adequacy of medical care;
•quality of medical equipment and services;
•patient, workforce, and public safety, as well as patient rights;
•qualifications and supervision of, and reimbursement for services provided by, medical and support personnel;
•the provision of services via telehealth, including technological standards and coverage restrictions, changes or other limitations on reimbursement;
•the confidentiality, maintenance, interoperability, exchange, and security of medical records and other health-related and personal information, including data breach, ransomware and identity theft issues;
•the development and use of AI and other predictive algorithms, including those used in clinical decision support tools;
•restrictions on the provision of medical care, including reproductive care;
•permitting, facility and personnel licensure, certification and accreditation requirements;
•enrollment standards and requirements for participation in government healthcare programs;
•corporate practice of medicine and fee-splitting;
•consumer disclosures and price transparency;
•the distribution, maintenance and dispensing of pharmaceuticals and controlled substances;
•relationships between healthcare providers and drug and medical device companies;
•debt collection, balance billing and billing for out of network services;
•translation services and accessibility requirements;
•communications with patients and consumers;
•advertising and marketing;
•operating policies and procedures;
•activities regarding competitors;
•insurance and the assumption of financial risk by healthcare entities, including allowable types of financial risk;
•addition of facilities and services; and
•environmental protections.
Among these laws are the Stark Law, the federal Anti-Kickback Statute, the FCA, the federal Civil Monetary Penalties Law, the Eliminating Kickbacks in Recovery Act, HIPAA, Health Information Technology for Economic and Clinical Health Act (“HITECH”), the Clinical Laboratory Improvement Amendments of 1988 (“CLIA”) and similar state laws. The Company, the Medical Groups and Privia Providers each have their own compliance obligations with respect to many of these laws and regulations, such as licensure and certification requirements to provide services and operate facilities and those related to billing and coding compliance. Although we provide general oversight and managerial support, to the extent permitted by applicable laws, and generally require compliance with laws under relevant contracts with the Medical Groups, we do not exercise control over the clinical decisions of practitioners and supervision of medical practice staff, and therefore we cannot provide assurance of their ongoing compliance.
Some healthcare laws apply to the financial relationships we have or our Medical Groups have with physicians and others who either refer or influence the referral of patients to our Medical Groups and Privia Providers or who are the recipients of referrals. The federal Anti-Kickback Statute, for example, is a criminal law that prohibits, among other things, the solicitation, receipt, offering or payment of any remuneration with the intent of generating referrals or orders for services or items that may be paid for by a federal healthcare program. The OIG has enacted safe harbor regulations that outline practices deemed protected from prosecution under the federal Anti-Kickback Statute. While we and our Medical Groups endeavor to comply with applicable safe harbors, certain current arrangements, including joint ventures and financial relationships with physicians and other referral sources and persons and entities to which our Medical Groups refer patients, may not qualify for safe harbor protection. Failure to qualify for a safe harbor does not mean the arrangement necessarily violates the federal Anti-Kickback Statute, but may subject the arrangement to greater scrutiny. We cannot offer assurance that practices outside of a safe harbor will not be found to violate the federal Anti-Kickback Statute. Allegations of violations of the federal Anti-Kickback Statute may also be brought under the federal Civil Monetary Penalty Law, which requires a lower burden of proof than other fraud and abuse laws.
The Stark Law is a strict liability civil law that prohibits physicians from making referrals for “designated health services” payable by Medicare or Medicaid to entities with which the physician or an immediate family member of the physician has a financial relationship, unless an exception applies. The Stark Law further prohibits entities that have received such referrals from filing claims with Medicare (or billing another individual, entity or third-party payer) for those referred services. The financial relationships of our Medical Groups with referring physicians and their immediate family members must comply with the Stark Law. We and our Medical Groups attempt to structure those relationships to meet an exception to or otherwise comply with the Stark Law, but the regulations implementing the Stark Law, including the requirements to meet exceptions, are detailed and complex. We do not always have the benefit of significant regulatory or judicial interpretation of the Stark Law and its implementing regulations. Thus, we cannot provide assurance that every relationship complies fully with the Stark Law. Unlike the federal Anti-Kickback Statute, failure to meet an exception under or otherwise comply with the Stark Law results in a violation of the Stark Law, even if such violation is technical in nature.
Additionally, violations of the federal Anti-Kickback Statute or Stark Law, improper billing for services to federal healthcare programs, or improper retention of overpayments from federal healthcare programs may be the basis for finding an FCA violation, either under a suit brought by the government or by a private person under a qui tam, or “whistleblower,” suit.
The data protection landscape is rapidly evolving, and the Company, its Medical Groups and ACO participants, are and may become subject to numerous state and federal laws, requirements and regulations governing the collection, use, disclosure, retention and security of health-related and other personal information. For example, the HIPAA privacy and security regulations extensively regulate the use and disclosure of PHI and require covered entities, including healthcare providers and health plans, and vendors (known as “business associates”) that perform certain services that involve creating, receiving, maintaining or transmitting PHI on behalf of covered entities or other business associates, to implement administrative, physical and technical safeguards to protect the privacy and security of PHI. These laws are complex and subject to change and interpretation, and our approach to compliance with such laws may include reliance on safe harbors or other regulatory rules, including those related to organized healthcare arrangements, which are themselves complex, require resources and investment to manage ongoing compliance, and are subject to change and interpretation, particularly in the current regulatory environment. In addition to HIPAA, there are numerous other laws, regulations, and legislative and regulatory initiatives at the federal and state levels governing the confidentiality, privacy, availability, integrity and security of health-related information and other types of personal information. In many cases, the state laws are more restrictive or impose more obligations than, and may not be preempted by, the HIPAA privacy and security regulations. State laws vary in scope, may apply to employees and business contacts in addition to patients, and may be subject to new and varying interpretations by courts and government agencies, creating complex compliance issues and potentially resulting in exposure to additional expense, adverse publicity and liability. The potential effects of these laws are far-reaching and may require the Company, its Medical Groups, and their third-party service and technology vendors to modify data use, storage, transmission and processing practices and policies, or our approach to compliance with other similar laws, and to incur substantial costs and expenses in order to comply. Failure by us or certain of our third-party vendors, including Privia Providers’ Affiliated Practices, to comply with these and any other comprehensive privacy laws passed at the state or federal level may result in regulatory enforcement action and reputational harm. We expect that new or modified laws, regulations, regulatory guidance and industry standards concerning privacy, data protection and information security, including those related to specific types of personal data, will continue to be proposed and enacted in various jurisdictions, which could impact our operations and cause us to incur substantial costs.
Additionally, the Telephone Consumer Protection Act (the “TCPA”) imposes specific requirements, including consent requirements and other restrictions, on communications with patients and consumers, including text messages or other communications that we or our Medical Groups may use to communicate with and perform outreach to our patients. TCPA violations can result in significant financial penalties, including penalties or criminal fines imposed by the Federal Communications Commission or through private litigation or by state authorities.
The Company and its Medical Groups are also subject to various federal and state antitrust laws that, for example, restrict exclusive contracting relationships with healthcare providers, restrict sharing of cost and pricing data, prohibit competitors from taking
collective action to set commercial payer reimbursement rates, and establish integration requirements (financial risk or clinical integration) for joint ventures or healthcare networks to jointly contract with payers.
If we or our Medical Groups fail to comply with these or other applicable laws and regulations, which are subject to change, any such failure could result in liabilities, including civil penalties; monetary damages; lapses in reimbursement; loss of facility licenses, accreditations, or certifications; revocation of billing privileges; exclusion of one or more entities and/or facilities from participation in the Medicare, Medicaid and other federal and state health care programs; termination of various relationships or contracts; lawsuits and criminal penalties. Medicare and Medicaid payments may be suspended pending even an investigation of what the government determines to be a credible allegation of fraud. We could also be required to make changes to our business model and/or practices, which could increase operating expenses, negatively impact our business relationships, and decrease access to new business opportunities. In addition, different interpretations or enforcement of, or amendments to, these and other laws and regulations in the future could subject current or past practices to allegations of impropriety or illegality or could require us to make changes in our operations, facilities, equipment, personnel, services, capital expenditures and operating expenses. The costs of compliance with, and the other burdens imposed by, these and other laws or regulatory actions may increase operational costs, result in interruptions or delays in the availability of systems and/or result in a decline in patient volume or Privia Provider, ACO participant or Medical Group attrition. Our failure to accurately anticipate the application of these laws and regulations to our business or any other failure to comply with current or future regulatory requirements could create liability for us and negatively impact our business. Any action against us for violation of these laws or regulations, even if we successfully defend against it, could cause us to incur significant legal expenses, divert management’s attention from the operation of our business or result in reputational harm, among other things.
Our business model relies on a complex legal framework that governs our relationships with Medical Groups and Privia Providers. Legal challenges or shifting interpretations of applicable laws could require us to make significant changes to our operations, which could adversely affect our business.
The structure of our business model is driven by nuanced legal concepts, some of which are subject to varying interpretations. Although we and our Medical Groups strive to comply with applicable federal and state laws and regulations, governmental authorities that administer these laws or other third parties may challenge our current structure.
At the state level, our ability to conduct business and the structure of our operations depends on each state’s laws, regulations, and policies governing, among other issues, the corporate practice of medicine, fee-splitting, and the assumption of financial risk. In several states, laws and regulations, guidance from professional licensing boards or state attorneys general and judicial doctrines prohibit corporations and other entities not owned by physicians or other permitted health professionals from practicing medicine and other professions. These laws and doctrines have been interpreted in some states to prohibit entities not owned by permitted professionals from employing physicians and other professionals and to prohibit such entities from undertaking activities that could be seen as exercising control over healthcare provider professional judgment. Some states also have adopted restrictions on direct or indirect payments to, or entering into fee-splitting arrangements with, physicians and unlicensed persons or business entities. These restrictions vary by state and are often vague and subject to interpretation by state medical boards, state attorneys general and other regulatory authorities. We attempt to structure our arrangements with healthcare providers to comply with applicable state law. However, we cannot provide assurance that governmental officials responsible for enforcing these laws will not assert that we, or transactions in which we are involved, violate these laws. These laws may also be interpreted by courts in a manner inconsistent with our interpretations. Possible sanctions for violations of these restrictions include the loss of a physician’s license and civil and criminal penalties. In addition, agreements between the Company and physicians may be considered void and unenforceable, our MSAs and management fees could be adversely affected, and we may be required to restructure the Company’s relationships with Medical Groups and Privia Physicians, any of which could have a material adverse effect on our business, financial condition and results of operations.
The structure of our business also is impacted by federal law. In particular, we seek to structure each Medical Group to comply with applicable Stark Law exceptions. We periodically review our Medical Groups and their relationships with Privia Physicians to ensure continued compliance and that the regulatory safeguards in various agreements are implemented appropriately. Despite our efforts, it is possible that governmental authorities may conclude that our business practices do not comply with the Stark Law and its implementing regulations, which could result in sanctions such as denial of payment, civil monetary penalties, and exclusion from federal healthcare programs. Further, we could be subject to significant repayment obligations, as the Stark Law requires entities to refund amounts received for items or services provided pursuant to a prohibited referral. Failure to timely repay such amounts may constitute a false or fraudulent claim and could result in civil penalties and additional penalties under the FCA.
If we or our Medical Groups are found to be in violation of the Stark Law or any other federal or state law affecting our business model or practices, we could be required to discontinue part of our current business or change our business structure, operations, or relationships with third-parties, such as Privia Providers, health system partners or payers, which may require us to incur significant costs. Any such changes could also negatively affect our business relationships, new business opportunities, and growth plans. In addition, our failure to accurately anticipate the application of various federal and state laws to our business or otherwise comply with legal requirements could result in significant legal expenses, divert management’s attention from the operation of our business, and result in adverse publicity, any of which could have a material adverse effect on our business.
Our business, financial condition and results of operations may be adversely affected by changes and uncertainty in the healthcare industry, including health reform initiatives and other changes to laws and regulations.
The healthcare industry is subject to changing political, regulatory and other influences, along with various scientific and technological initiatives and innovations. Regulatory uncertainty has increased as a result of decisions issued by the U.S. Supreme Court in June 2024 that affect review of federal agency actions, including Loper Bright Enterprises v. Raimondo. These decisions increase judicial scrutiny of agency authority, shift greater responsibility for statutory interpretation to courts and expand the timeline in which a plaintiff can sue regulators, all of which could have significant impacts on government agency regulation, particularly within the heavily-regulated healthcare industry, and may have broad implications for our business. While the effects of these decisions will become apparent over the coming months and years, we anticipate an increase in legal challenges to healthcare regulations and agency guidance and decisions, including but not limited to those issued by HHS and certain of its agencies, such as the CMS, FDA, and OIG. Federal agencies oversee, regulate and otherwise affect many aspects of our business, including through Medicare and Medicaid payment and coverage policies, policies affecting size of the uninsured population, administration of state Medicaid programs, and enforcement and interpretation of fraud and abuse laws. In addition to increased uncertainty and potential changes to regulations and agency guidance as a result of legal challenges, the recent U.S. Supreme Court decisions may result in inconsistent judicial interpretations and delays in and other impacts to the agency rulemaking and legislative processes, among other effects, any of which could require us to make changes to our operations that may have a materially negative impact on our business.
The healthcare industry has been and continues to be impacted by healthcare reform efforts. For example, the Affordable Care Act (“ACA”) affects how healthcare services are covered, delivered and reimbursed and expanded health insurance coverage through a combination of public program expansion and private sector health insurance reforms. Changes in the law’s implementation, subsequent legislation and regulations, state initiatives and other factors, including changes to the ACA such as those contained in the One Big Beautiful Bill Act of 2025 (“OBBBA”), have affected, and may continue to affect, the number of individuals that elect to obtain public or private health insurance or the scope of such coverage. Reductions in the number of insured individuals, as well as the scope of insurance coverage may have an adverse effect on our business. In addition, Medicare and Medicaid policies and programs, such as MSSP, are subject to change, including as a result of changes in the presidential administration and Congress. Legislation and administrative actions at the federal level, including those taken by CMS or the Center for Medicare and Medicaid Innovation, may impact funding for, or the structure of, the Medicaid or Medicare program, and may shape administration of the Medicaid program at the state level and Medicare Advantage Programs. Additionally, funding for scientific research may be impacted by legislation or administrative actions at the federal level, which in turn may impact the availability of and need for clinical research programs in which Privia Providers participate. Other recent health reform initiatives and proposals at the federal and state levels include those focused on price transparency and out-of-network charges as well as pharmacy and pharmacy benefit manager reform efforts, which may impact prices, the relationships between hospitals, patients, payers, and providers, total cost of care and patient outcomes, and lead to further uncertainty in other participants in the healthcare industry, including employers. Other industry participants, such as private payers and large employer groups and their affiliates, have implemented and may in the future introduce additional financial or delivery system reforms.
There is uncertainty regarding whether, when, and what other health reform initiatives will be adopted through governmental avenues and/or the private sector, the timing and implementation of any such efforts, and the impact of those efforts on providers as well as other healthcare industry participants. It is difficult to predict the nature and/or success of current and future health reform initiatives, any of which may have an adverse effect on our business, financial condition, results of operations, cash flow, capital resources and liquidity.
We, our Medical Groups and Privia Providers, may be subject to legal proceedings, including litigation, governmental investigations and claims, and payer audits.
The Company, its Medical Groups, and Privia Providers have been and may become subject to various legal and governmental proceedings. The Company, its Medical Groups and Privia Providers may face allegations and claims, including those that improperly name the Company or its Medical Groups as parties to the proceeding, related to various topics, including billing and coding for healthcare services and other reimbursement issues, malpractice, data privacy and security, labor and employment, consumer protection, intellectual property infringement, misappropriation and other issues, including those related to our acquisitions, securities issuances or business practices. These matters may include claims for substantial or indeterminate amounts of damages and claims for injunctive relief. If an unfavorable outcome occurs in connection with any current or future legal proceedings or other loss contingencies, we or our Medical Groups may be subject to significant settlement costs or judgments, penalties, reputational harm, and/or requirements to modify or limit our operations or services, any of which could negatively impact our business, operations, and growth strategy. Managing legal proceedings, even if the outcomes are favorable, can be time- and resource-consuming, be disruptive to normal business operations, divert management’s attention from the business and result in adverse publicity and reputational harm.
Healthcare companies, in particular, are subject to various reviews, investigations and audits by governmental authorities to verify compliance with applicable laws, regulations, and Medicare and Medicaid program requirements. Both federal and state governmental agencies have heightened civil and criminal enforcement efforts in recent years and expanded collaborative program integrity initiatives. These efforts have led to a number of investigations, prosecutions, convictions and settlements in our industry in general, including under federal civil and criminal false claims laws. Further, under the FCA and some similar state laws, private parties may
bring whistleblower lawsuits against companies that allegedly submit false claims for payments to, or improperly retain overpayments from, the government.
Government agencies, including the OIG, CMS and their agents, such as Medicare administrative contractors (“MACs”), may conduct audits of our and our Medical Groups’ operations. CMS and state Medicaid agencies contract with recovery audit contractors (“RACs”) and other contractors to conduct post-payment reviews to detect and correct improper payments in the Medicare program, including Medicare Advantage, and the Medicaid programs. Other third-party payers may conduct similar audits. In addition, we and our Medical Groups perform internal audits and monitoring. Depending on the nature of the conduct found in audits and investigations and whether the underlying conduct could, for example, be considered systemic, knowing or intentional, their resolution could have a material, adverse effect on our operations and financial position or result in adverse publicity and reputational harm. Further, negative audit findings or determinations that our, our Medical Groups’ or ACOs’ operations violate applicable laws and regulations may result in repayment obligations or recoupment of previously paid claims, payment suspension or the revocation of billing or payment privileges, corporate integrity agreements, and civil and criminal penalties, including significant fines and damages and other sanctions, such as exclusion from governmental healthcare programs, any of which could have an adverse effect on our business, operations, and financial condition or result in adverse publicity and reputational harm.
Although the Company, its Medical Groups and/or Privia Providers maintain third-party professional liability insurance coverage, claims against us could exceed the coverage limits of our insurance policies or particular claims could be excluded from coverage. Professional liability claims in excess of applicable insurance coverage could have a materially adverse effect on our business, financial condition, reputation, and results of operations. In addition, any professional liability claim brought against us, our Medical Groups or Privia Providers, with or without merit, could result in an increase of professional liability insurance premiums. Insurance coverage varies in cost and can be difficult to obtain, and we cannot guarantee that we, our Medical Groups or Privia Providers will be able to obtain insurance coverage in the future on terms acceptable to us or at all. If our costs related to insurance and claims increase, our business and financial condition could be adversely affected.
Risks Related to Our Business and Operations
Risks associated with VBC arrangements may negatively impact our business, operations, and financial condition.
A significant portion of our business is derived from VBC arrangements for healthcare services, including MSSP, Medicare Advantage and commercial VBC arrangements. Generally, VBC contracts tie incentive payments to specific targets for risk adjusted total cost of care, quality related process and outcome measures, and beneficiary experience of care. The VBC revenues of the Company, its Medical Groups, and ACOs are subject to risks including managing established, and any changes to, targets relative to utilization by patients, unit cost and the mix of healthcare services; annual fluctuations in payment terms for certain VBC arrangements, such as Medicare Advantage payment rates and care coordination fees; changes in patient attribution and attribution methodologies; and changes in plan design and other terms by payers. CMS has developed several alternative payment models (“APM”s) that use VBC contract structure to incentivize cost-efficient and high-quality care for Medicare beneficiaries, including ACOs and bundled payment models. There are also state-driven and third-party payer VBC initiatives. For example, some states have implemented APMs or aligned quality metrics across payers. Many private third-party payers are also transitioning toward APMs or implementing other VBC strategies. For example, many large private third-party payers, such as managed care plans, currently require physicians to report quality data. While participation in such APMs, including ACOs, has historically been voluntary, CMS and certain other payers have indicated that participation in future programs may be required, and any changes to or elimination of VBC arrangements by CMS or other payers (including, for example, to prospective trend targets, risk adjusted regional efficiency, or the requirements for participation) could have a material adverse effect on our business, results of operations, financial condition and cash flows.
Regulation of risk-sharing arrangements, including certain VBC arrangements, varies significantly by state. If a state in which we currently operate, or in which we seek to expand, views the participation of the Company, its Medical Groups, clinically integrated networks, or ACOs in risk-sharing arrangements as the assumption of insurance risk, the arrangement may fall within the purview of state insurance or managed care laws and regulations, and we, the Medical Group or ACO may be required to obtain a state insurance or managed care license or similar registration. These laws and regulations may subject the entity involved to oversight by state regulators, including through periodic reporting or audits, and requirements for financial reserves. Some of these laws may be vague and state regulators may have interpretations that differ from ours. Even if a state regulatory agency does not directly oversee the transfer of risk by a payer to a downstream entity, the state may require the licensed payer to include certain oversight mechanisms in payer contracts, which could increase our, our Medical Groups’ or ACOs’ administrative costs and have an adverse effect on our business, cash flows or results of operations. If we, our Medical Groups or ACOs fail to comply with insurance laws and regulations, including licensure and oversight requirements, we may be required to make changes to our operations and could be subject to civil and/or criminal penalties, denial of future licensure applications and termination of payer contracts. These laws and regulations may affect the operation of, for example, ACOs, direct primary care programs, provider-sponsored organizations, independent practice associations, clinically integrated networks, and provider capitation models.
Success in VBC contracts requires coordination of teams and a combination of data, analytics, software-supported workflow management and automation in addition to direct patient interaction. We are dependent on Privia Providers and other providers
affiliated with our ACOs to effectively manage the quality and cost of care, and we cannot guarantee nor control the quality and efficiency of services from such providers or the attrition of providers, including those with a track record of success in VBC arrangements, or attributed participants. While we believe we are well-positioned to compete in a value-based reimbursement environment and facilitate the transition from FFS models to VBC arrangements, it is unclear whether VBC arrangements will ultimately achieve their aims and whether they will decrease aggregate reimbursement. If we, our Medical Groups, or ACOs fail to achieve contract performance standards under any applicable VBC program, perform at a level below the outcomes demonstrated by our competitors, or otherwise fail to effectively provide or coordinate the efficient delivery of quality health care services, our reputation in the industry may be negatively impacted, we may receive reduced reimbursement amounts, including the loss of shared savings or other bonuses, and we may owe repayments to payers, causing our revenues to decline and leading to dissatisfaction among providers. In addition, failure to satisfy qualify performance standards may lead to the termination of a physician’s ability to participate in a particular commercial payer product or result in our Medical Groups not being able to participate in a particular VBC arrangement, tiered network or narrow network offering. Reductions in the quality of services furnished by our Medical Groups, Privia Providers or ACO participants could have a materially adverse effect on our business, results of operations, financial condition and cash flows.
Additionally, the Company monitors and manages quality metrics, including star ratings for Medicare Advantage plans, and submits quality data on behalf of its Medical Groups, as well as its ACO participants. Any delays or inaccuracies in information from payers or issues with the quality or integrity of data from third-parties, including as a result of the highly complex process required to summarize, organize and deliver actionable data to Privia Providers, may prevent us, our Medical Groups or ACO participants, from making necessary changes to mitigate potential quality concerns, attribution changes or total cost of care. As more of our and our Medical Groups’ revenues are derived from VBC arrangements, actuarial modeling and effective strategies to appropriately control costs and expenses are necessary for success, and any failure by us or our Medical Groups to adequately predict and control our and the Medical Groups’ costs and expenses and to make reasonable estimates and maintain adequate accruals for VBC revenues or incurred but not reported claims, could have a material adverse effect on our business, results of operations, financial condition and cash flows. Furthermore, to the extent that our Medical Groups’ patients require more care than anticipated or our medical costs and expenses exceed estimates, reimbursement paid under our VBC arrangements may be insufficient to cover costs. This may negatively impact both our revenue from Medical Groups and from management services furnished to Non-Owned Medical Groups. Although we seek to mitigate some of this risk on a case-by-case basis with stop-loss insurance coverage, we generally have little ability to increase our coverage during the terms of our VBC arrangements.
If federal or state healthcare programs or commercial payers reduce reimbursement rates we receive or alter payment terms, if we and our Medical Groups are unable to retain and negotiate favorable contracts with private third-party payers, if insured individuals move to health plans with greater coverage exclusions or restrictions or narrower networks, or if our Medical Groups’ volume of uninsured or underinsured patients increases, our revenues may decline.
The revenues of the Company and its Medical Groups depend significantly on reimbursement by governmental and private third-party payers. Federal and state governments have made, and continue to make, significant changes to the Medicare and Medicaid programs, including reductions in reimbursement levels and eligibility requirements. For example, CMS makes annual updates to its Medicare Physician Fee Schedule, including modifications to the Quality Payment Program. Reductions in payments under government healthcare programs may also negatively impact payments from private third-party payers because, in some cases, third-party payers rely on all or portions of Medicare payment systems to determine payment rates. In addition, the VBC revenues of the Company and our Medical Groups are subject to risks involving annual fluctuations in payment terms for certain VBC arrangements, such as care coordination fees or Medicare Advantage payment rates, changes in patient attribution, and changes in plan design and other terms by payers. For example, CMS regularly updates its Medicare Advantage risk adjustment model, the CMS Hierarchical Condition Categories (“HCC”) model, to account for healthcare utilization and cost data, including by recalibrating the model with newer data, updating condition categories or diagnosis codes, and adjusting to coding pattern differences. Changes and variations in the HCC model impact risk scores and payer revenue, which in turn could significantly affect the payments providers receive, and, as a result, adversely impact our business and results of operations.
Private third-party payers, including managed care plans, may reimburse healthcare providers at a higher rate than Medicare, Medicaid or other government healthcare programs, depending on a variety of factors. Reimbursement rates are set forth by contract when providers are in-network. Our and our Medical Groups’ typical agreements with commercial payers only secure reimbursement rates for, generally, a period of one to three years. The ongoing trend toward consolidation among payers tends to increase their bargaining power over fee structures, and third-party payers continue to demand discounted fee structures. Payers may also utilize plan structures such as narrow networks and tiered networks that limit members’ provider choices, impose significantly higher cost sharing obligations when care is obtained from providers in a disfavored tier or otherwise shift greater financial responsibility for care to patients, and such plan structures could be disadvantageous to Privia Providers. If any commercial payers reduce their reimbursement rates, elect not to cover some or all of the healthcare services our Medical Groups provide, restrict our ability to add new providers or participate in new products or plans, or restrain the ability of Privia Providers to furnish services to patients through plan structures or cost control strategies, our business may be harmed.
Our future success will depend, in part, on our and our Medical Groups’ ability to retain and renew our third-party payer contracts and enter into new contracts on favorable terms. The contracts we and our Medical Groups have with payers require us to comply with a number of terms related to the provision of services and billing for services. If we or our Medical Groups are unable to negotiate increased reimbursement rates, maintain existing rates or other favorable contract terms (including when adding new providers to existing arrangements), effectively respond to payer cost controls or comply with the terms of the payer contracts, the payments we and our Medical Groups receive for services may be reduced and we may be involved in payer disputes and experience payment denials, both prospectively and retroactively. If a payer terminates or elects not to renew its relationship with us or our Medical Groups, our ability to retain patients associated with that payer is limited and consequently could have a material adverse effect on our business, results of operations, financial condition and cash flows. Payers, including those offering Commercial, Medicare Advantage, Medicaid, TriCare and ACA plans have become increasingly aggressive in attempting to minimize the use of out-of-network providers by disregarding the assignment of payment from their enrollees to out-of-network providers (i.e., sending payments directly to members instead of to out-of-network providers), capping out-of-network benefits payable to members, waiving out-of-pocket payment amounts and initiating litigation against out-of-network providers for interference with contractual relationships, insurance fraud and violation of state licensing and consumer protection laws. Many states have laws and regulations that prevent providers from waiving patient out-of-pocket amounts, including out-of-network charges, when such providers submit their full charges to payers. To the extent that we, our Medical Groups or Privia Providers are not able to enter into contracts on favorable terms with payers, including with respect to in-network or out-of-network designations, our patient volumes may suffer and our revenues may decline.
Our revenues and the relationships we and our Medical Groups have with payers may also be impacted by price transparency initiatives. For example, HHS requires health insurers to publish online charges negotiated with providers for healthcare services, which could impact our negotiations with payers. In addition, the No Surprises Act places limitations on billing for certain services furnished by providers who are not in-network with the patient’s health plan, among other requirements. Price transparency initiatives may impact the ability of the Company and our Medical Groups to set and negotiate prices and the relationships between healthcare providers, payers and patients, which may reduce our revenues.
Changes in payer mix could adversely affect the overall reimbursement we and our Medical Groups receive from payers. Such changes could be driven by an economic downturn that results in more uninsured patients or patients insured by state Medicaid programs, among other factors. Failure of any federal or state government to make payments under the Medicare and Medicaid programs could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows. Further, any failure by the United States Congress to complete the federal budget process and fund government operations may result in a federal government shutdown, potentially causing us to incur substantial costs without reimbursement under the Medicare program, which could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows. If we or our Medical Groups experience changes in payer mix or reductions in reimbursement, have payer contracts that are not competitive in a given market or are unable to obtain or maintain contracts with certain payers, our revenues could decrease and our ability to recruit new physicians may be adversely impacted, which could adversely affect our growth strategy and financial projections.
An increase in the volume of uninsured patients or deterioration in the collectability of patient responsibility accounts could adversely affect our financial condition and results of operations.
There are collection risks related to our and our Medical Groups’ uninsured patient accounts and patient accounts for which the patient responsibility amounts (e.g., deductibles, copayments, coverage exclusions) remain outstanding. Any increase in the volume of uninsured patients or deterioration in the collectability of uninsured and self-pay accounts receivable could adversely affect our cash flows and results of operations.
We and our Medical Groups may experience growth in uninsured patients as a result of a number of factors, including macroeconomic conditions, changes to ACA subsidies and Medicaid eligibility under the OBBBA, and unemployment levels. In addition, federal and state legislatures have in recent years considered or passed various proposals impacting the size of the uninsured or underinsured population. Further, participation in Medicaid programs continues to evolve. For example, following the expiration in 2023 of early COVID-19-related legislation that had the effect of expanding Medicaid coverage, Medicaid enrollment has continued to decline through 2025 in light of continued Medicaid redeterminations and changes to eligibility requirements under the OBBBA. In addition, some states have imposed individual health insurance mandates and other states have explored or offer public health insurance options. These variables, among others, make it difficult to predict the size of the uninsured population and what percentage of our total revenue will be comprised of self-pay revenues.
We may also be adversely affected by the growth in patient responsibility accounts as a result of increases in the adoption of health plan structures, including health savings accounts and narrow or tiered networks, that shift greater payment responsibility for care to individuals through greater exclusions and copayment and deductible amounts. Further, the ability of the Company and its Medical Groups to collect patient responsibility accounts may be limited by statutory, regulatory and investigatory initiatives. For example, the No Surprises Act requires providers to send uninsured and self-pay patients a good faith estimate of expected charges for items and services and provides a dispute process for bills that exceed the good faith estimate by certain predetermined amounts.
A deterioration of economic conditions in the United States could lead to higher levels of uninsured patients, result in higher levels of patients covered by lower paying government programs, result in fiscal uncertainties for both governmental and commercial payers, or limit the economic ability of patients to make payments for which they are responsible. If we and our Medical Groups experience growth in self-pay volume or deterioration in collectability of patient responsibility accounts, our financial condition or results of operations could be adversely affected.
The reimbursement process is complex and may involve delays and other uncertainties, which may adversely affect our business, operations, cash flows, revenues, and earnings.
The Company and its Medical Groups may encounter significant delays and other uncertainties under both FFS and VBC reimbursement models, which could adversely affect our business and financial condition. The billing and collection process is complex and varies across states and among payers, including as a result of frequent insurance coverage changes, geographic coverage differences, differing interpretations of contract coverage and other payer and provider issues, such as ensuring appropriate documentation. Third-party payers may disallow, in whole or in part, requests for reimbursement based on determinations that the patient is ineligible for coverage, other coverage exclusions or determinations that services were not medically necessary or not adequately documented. We and our Medical Groups are subject to commercial and governmental payer audits and may be required to make repayments based on the findings of those audits. In addition, determining applicable primary and secondary coverage for our patients is a complex, resource-intensive process, and errors in coordination of benefits determinations may result in refunds to payers. Revenues are subject to estimating risk as a result of the complexity of the billing and collection process, including related to determining amounts not paid by the primary payer that will ultimately be collectible through secondary coverage or from the patient. Retroactive adjustment by, and refunds to, payers may change amounts realized and recognized as revenue from third-party payers.
Further, there can be lengthy delays between the provision of services and ultimate payment. Under VBC arrangements, payment of any shared savings, bonuses, withholds and similar payments is received only after the close of the relevant measure period (e.g., calendar year), and only after the payer has reconciled cost of care, FFS reimbursement paid, as applicable, reported quality data, and patient attribution. Delays and uncertainties in the reimbursement process may adversely affect accounts receivable, increase the costs of collection and cause us to incur additional borrowing costs.
Before receiving reimbursement from governmental healthcare programs and commercial payers under either FFS or VBC models, we, our Medical Groups and Privia Providers must be appropriately enrolled and credentialed with the relevant programs and payers. Enrollment rules, including limitations on retroactive billing, vary by program. If we or our Medical Groups do not enroll a Privia Provider in a timely manner, the Medical Group may be precluded from billing for any services rendered to a beneficiary prior to the effective date of enrollment. Failure to timely or accurately submit required information to payers may result in reimbursement delays or denials that could result in adverse financial impacts to Privia Providers’ medical practices (leading to attrition) or adversely affect our operations, cash flows and revenues, and CMS may impose penalties on providers that submit incomplete or inaccurate information. Further, providers are generally required to periodically revalidate enrollment and credentialing information and provide updates to payers of significant changes. Failure to comply with these and other requirements could result in revocation of enrollment and billing privileges and denial of future applications.
The information that we or our Medical Groups provide to Medicare Advantage plans and other payers could be inaccurate, incomplete or unsupportable, which could impact risk adjustment scores and ultimately result in harm to our business, operations and financial condition.
The Company (on behalf of some Medical Groups) and its Medical Groups submit claims and encounter data to Medicare Advantage plans and other payers that are used to establish Risk Adjustment Factor (“RAF”) scores attributable to beneficiaries. The RAF scores impact the revenue that the health plans and, in turn, our Medical Groups are credited with for the provision of medical care to these patients. The data submitted to CMS by each health plan are based partially on medical charts and diagnosis codes that our Privia Providers prepare and we submit to the health plans. Each health plan generally relies on us and our Privia Providers to appropriately document and support the RAF-related data in our medical records and to accurately code claims for medical services provided to members. Although we, our Medical Groups and our payers have implemented auditing and monitoring processes to collect and provide accurate risk adjustment data to CMS, these efforts may not be sufficient to ensure the accuracy of such data. Erroneous claims, encounter records and submissions to Medicare Advantage plans could result in inaccurate revenue and risk adjustment payments, which are subject to correction or retroactive adjustment in later periods. This corrected or adjusted information may be reflected in financial statements for periods subsequent to the period in which the revenue was recorded. We or our Medical Groups may be required to refund a portion of revenues received, which depending the magnitude of the refund, could damage our relationships with the applicable health plan and could have a material adverse effect on our business, results of operations, financial condition and cash flows.
Medicare Advantage plans are subject to audit by government agencies. CMS audits Medicare Advantage plans for documentation to support RAF-related payments for enrollees through its Risk Adjustment Data Validation (“RADV”) audits, and may seek repayment based on audit findings. CMS has indicated that payment adjustments will not be limited to RAF scores for the specific Medicare Advantage enrollees for which errors are found, but may also be extrapolated to the entire Medicare Advantage plan subject to a particular CMS contract. In February 2023, CMS published a final rule updating the RADV audit methodology used by CMS to
address overpayments to Medicare Advantage plans based on the submission of unsupported risk-adjusting diagnosis codes. The 2023 final rule was recently vacated following legal challenges, which may result in additional uncertainty around the framework for RADV audits in the future. The OIG conducts audits of Medicare Advantage plans that are similar to RADV audits, addressing diagnoses collected and submitted to CMS for risk adjustment purposes. In addition, there is increasing scrutiny by the Department of Justice (“DOJ”) with regard to RAF scores, as the agency has intervened in litigation under the FCA related to RAF scores. Medicare Advantage plans with which we or our Medical Groups contract may be selected for review by CMS, OIG, DOJ or another government agency or its contractor, and the outcome of such actions may result in material adjustments to our revenues. A Medicare Advantage plan may seek repayment from us, our Medical Groups or our ACOs if CMS, the OIG or another government entity makes any payment adjustments to the Medicare Advantage plan as a result of the audit and assessment of RAF scores that were supported by our data or the data of our Medical Groups.
Moreover, we, our Medical Groups or our ACOs may face civil and criminal liability under healthcare fraud and abuse laws, including the FCA, which can result in significant penalties. Further, Medicare Advantage plans may seek to hold us liable for any penalties they owe under the FCA or other fraud and abuse laws as a result of inaccurate or unsupportable data provided by us. The DOJ has asserted FCA claims against, and entered into settlement agreements or corporate integrity agreements including significant civil monetary penalties with, Medicare Advantage plans and providers related to maintaining internal coding policies and provider education that allegedly resulted in the submission of inappropriate diagnosis codes, the inappropriate capture of historical diagnoses that inflated the organization’s RAF scores and resulted in inflated payment rates, submission of inaccurate information about the health status of beneficiaries enrolled in Medicare Advantage plans and failure to remove diagnosis codes that were no longer applicable or supported by the chart review.
There can be no assurance that a Medicare Advantage plan in which our Medical Groups participate will not be randomly selected or targeted for review by CMS or that the outcome of such a review will not result in a material adjustment in our revenue and profitability, even if we believe the information we submitted to the plan is accurate and supportable. Further, although we have built safeguards into our provider education efforts and unreported diagnoses review, there can be no assurance that CMS, the DOJ, the OIG, or a whistleblower would not allege such action constitutes a civil FCA violation or that we could successfully defend against such allegation. Even if we are successful, defending against such a claim could cause us to incur significant legal expenses, divert our management’s attention from the operation of our business and result in reputational harm, any of which could adversely affect our business.
Third-party payer controls designed to reduce costs and other payer practices to decrease or review utilization, surgical procedure volumes or reimbursement for services rendered may reduce our revenues.
Controls imposed by Medicare, Medicare Advantage, Medicaid, managed Medicaid and private third-party payers, including through the use of AI, that are designed to reduce the intensity of services and surgical volumes, in some instances referred to as “utilization review,” have affected and are expected to increasingly affect our Medical Groups and Privia Providers. Utilization review entails the review of the course of treatment of a patient by third-party payers, and may involve prior authorization requirements. The Medicare program also issues national or local coverage determinations that restrict the circumstances under which Medicare pays for certain services and, starting in 2026, is implementing its own prior authorization process. Cost control efforts, including coverage restrictions, have resulted in an increase in reimbursement denials and delays by governmental and commercial payers, which may increase costs and administrative burden for the Company, our Medical Groups and Privia Providers and decrease the reimbursement we and our Medical Groups receive. Efforts by payers to impose more stringent cost controls are expected to continue and may have a material, adverse effect on our business, financial condition, and results of operations.
If the Company and its Medical Groups are unable to effectively compete, our business, financial condition, and results of operations could be adversely impacted.
The healthcare industry is highly competitive and we expect competition to continue to increase. We and our Medical Groups compete with healthcare service providers, management services organizations, physician enablement entities, and provider networks, intermediary entities, data consultants, payers, and other companies managing and facilitating FFS and VBC arrangements through tools, talent and technology-enabled, nationally-focused business models. Some of our competitors may have greater financial, technical, political, and marketing resources, name recognition, broader or more effective service offerings, or a larger number of patients, customers, or payers than we do. In addition, some of our competitors have been in business longer than we have or may have more mature or effective tools, strategies and procedures. Generally, other medical groups and healthcare providers in the markets our Medical Groups serve provide services similar to those our Medical Groups offer, but some competing providers may be more established, have higher caliber facilities and equipment, be located in areas that are easier to access, and offer better access to and a broader array of specialties and services. These competitive advantages may limit the ability of the Company and its Medical Groups to attract and retain skilled talent, patients, and providers in local markets and to expand into new markets. In addition, we and our Medical Groups may face competition from new entrants into our markets. Competition for patients and providers may adversely affect contract negotiations and performance as well as patient volumes and other aspects of our business.
Trends toward performance data and price transparency may impact the competitive position and patient volumes of the Company and its Medical Groups. CMS websites make publicly available certain data on ACOs and on clinicians, medical groups, and various other
types of Medicare-enrolled providers, including QPP performance information. If Privia Providers, our Medical Groups, or ACOs achieve poor results (or results that are lower than competitors’ results) on performance metrics, our competitive position could be negatively affected, and we may attract fewer patients or providers. In addition, HHS requires health insurers to publish online charges negotiated with providers for healthcare services, and health insurers must provide online price comparison tools to help individuals get personalized cost estimates for covered items and services. The No Surprises Act also requires providers to send uninsured or self-pay patients (in advance of the date of the scheduled item or service or upon request) and health plans (prior to the scheduled date of the item or service) of insured patients a good faith estimate of the expected charges and diagnostic codes. Until additional regulations are issued, HHS is deferring enforcement of certain No Surprises Act requirements related to good faith estimates, including the requirement that estimates provided to uninsured or self-pay patients include expected charges for co-providers or co-facilities. It is not entirely clear how price transparency requirements will affect consumer behavior, relationships between payers and providers, or the ability of providers to set and negotiate prices, but our competitive position and the competitive position of our Medical Groups could be negatively affected if prices are higher or perceived to be higher than those of our competitors.
Industry consolidation may also negatively impact the competitive position of the Company and its Medical Groups. Other healthcare industry participants, including payers, are increasingly facilitating VBC arrangements and implementing physician alignment strategies, such as employing physicians, acquiring physician practice groups, participating in ACOs or other clinical integration models. We and our Medical Groups compete for payer relationships with other physician practices and intermediary entities such as non-Privia ACOs, independent physician associations and physician hospital organizations. There is increasing consolidation in the third-party payer industry, including the vertical integration of health insurers with providers, and increasing efforts by payers to influence or direct a patient’s choice of provider by the use of narrow networks or other strategies. Some payers have developed their own managed services tools, which they may offer to large numbers of physicians. Insurers may have increased negotiating leverage and other competitive advantages, such as greater access to performance and pricing data, as a result of consolidation within the industry. Consolidation within the third-party payer industry may negatively affect the ability of the Company and its Medical Groups to negotiate prices and favorable terms with health insurers, as well as our ability to successfully market our services to providers. Other healthcare industry participants, such as large employer groups and their affiliates, may intensify competitive pressure and affect market dynamics in ways that are difficult to predict.
If competitors are better able to attract patients or providers, make capital expenditures, maintain or upgrade facilities and equipment, recruit or align with physicians, expand services, innovate, obtain and perform in favorable third-party payer contracts, including VBC arrangements, we and our Medical Groups may experience a decline in patient and provider volumes. If we are unable to successfully compete, our business, financial condition, cash flows, and results of operations could be materially adversely affected.
If we do not continue to innovate and evolve our service offerings in a way that is useful to our Medical Groups, Privia Providers and their patients, our health system or hospital partners, and third-party payers, we may not remain competitive, fail to meet our growth expectations, and our revenue and results of operations could suffer.
We believe that the market for healthcare in the United States is in the midst of structural change, with an increased emphasis on VBC models, technological solutions and a customer-centered focus. Our success depends on our ability to keep pace with technological developments (including the use of AI), satisfy increasingly sophisticated physician, payer and patient requirements, and the market continuing to evolve towards a VBC model. Our future financial performance will depend in part on growth in the healthcare market and on our ability to adapt to emerging demands of the market, including adapting to the ways our Medical Groups, Privia Physicians and their patients, our health system and hospital partners, and third-party payers interact with the Privia Technology Solution, the Privia Platform, and our operating model. Our competitors are constantly developing products and services that may be more efficient or appealing to Medical Groups, Privia Providers and their patients, our health system or hospital partners or third-party payers. To compete, we must continue to invest significant resources in research and development in order to enhance our existing service offerings and introduce new high-quality services and applications that such customers will want, while offering and operating the Privia Technology Solution and Privia Platform at competitive prices. If we fail to accurately predict customer preferences related to functionality, or industry changes needed to service our customers including providers, beneficiaries, and payers, or if we are unable to modify our service offerings on a timely or cost-effective basis, we may lose Medical Groups, Privia Providers, patients, health system or hospital partners, ACO participants and payer relationships. Our results of operations could also suffer if our innovations do not produce the desired results including related to contract performance, are not appropriately responsive to the needs of our multiple stakeholders, are not appropriately timed with market opportunity, or are not effectively brought to market, including as the result of delayed releases or releases that are ineffective or have errors or defects. As technology continues to develop, our competitors may be able to offer results that are, or that are perceived to be, substantially similar to, or better than, those generated by the Privia Technology Solution, the Privia Platform, or the Privia operating model. We may be required to compete on additional service attributes and to expend significant resources in order to remain competitive. If we are unable to successfully compete, our business, financial condition, and results of operations could be materially adversely affected.
Our sales and implementation cycle can be long and unpredictable and requires considerable time and expense, which may cause our results of operations to fluctuate.
The sales cycle for physicians and non-physician practitioners to become affiliated with our Medical Groups from initial contact with a potential lead to contract execution, varies widely and is unpredictable. Further, once a physician has executed the agreements
associated with one of our Medical Groups, there is a long period of implementation where the physician and his or her staff are trained on our EMR, platform and workflows and credentialed or enrolled in payer arrangements, as applicable. During such implementation period, we are incurring costs associated with the implementation without any corresponding revenue. Our sales efforts involve educating potential Privia Providers about our model, market offerings, the health care industry and the physician practice’s expected return on investment from becoming affiliated with the Medical Group. It is possible that in the future we may experience even longer sales cycles, especially with respect to moving into new geographic markets and as markets become more mature and concentrated, which could result in more upfront sales costs and less predictability in closing our Privia Physician sales. If our sales cycle lengthens or our substantial upfront sales and implementation investments do not result in sufficient sales to justify our investments, it could have a material adverse effect on our business, financial condition and results of operations.
As we expect to grow rapidly, our clinician recruitment costs could outpace our build-up of recurring revenue, and we may be unable to reduce our total operating costs through economies of scale such that we are unable to achieve profitability. Any increased or unexpected costs or unanticipated delays in taking a Privia Physician live on the Privia Technology Solution, including delays caused by factors outside our control, could negatively impact our reputation and/or our relationships with Privia Providers and cause our operating results and growth targets to suffer and negatively affect our revenue and profits.
Our ability to efficiently price the Privia Technology Solution, the Privia Platform, and our Privia operating model could affect our results of operations and our ability to attract or retain Medical Groups, Privia Physicians, health system or hospital partners, ACO participants and payers.
The management and administrative fees we charge our Medical Groups are generally set as a percentage of the Non-Owned Medical Group’s FFS collections provided such an arrangement is allowed under state fee splitting laws. Certain states restrict percentage management fees and, therefore, certain markets are structured as a fixed annual amount. Generally, if Privia offers additional, optional services, Privia Physicians enter into a separate agreement to purchase such services. We determine these prices based on factors such as prior experience, the costs inputs associated with the services, market competition and feedback from our Medical Groups, Privia Physicians, health system or hospital partners and ACO participants, our assessments may not be accurate and we could be underpricing or overpricing the Privia Technology Solution, the Privia Platform, and our operating model. Additionally, fees must generally be fair market value under federal and state fraud and abuse laws such as the federal Anti-Kickback Statute and the Stark Law. From time to time, we may choose to, or be required to, adjust our pricing, particularly as our applications and service offerings evolve. Changes to our pricing model or our inability to efficiently price our services could harm our business, results of operations, and financial condition and impact our ability to predict our future performance.
Our performance depends on our ability to contract with Medical Groups, Privia Providers, health system partners, ACO participants and third-party payers.
Our business and operating model depend on our relationships with Medical Groups, Privia Providers, health system partners, ACO participants and payers. We typically enter into multiyear contracts with our Medical Groups, Privia Providers, health system partners, ACO participants and payer customers. We expect to derive a significant portion of our revenue from renewal of existing contracts, including through the expansion of our service offerings, including existing and new offerings, such as ancillary services, additional medical and medical support services like our virtual visits platform and clinical research program. Achieving high retention rates and selling additional applications and services are critical to our future business, revenue growth and results of operations.
Factors that may affect our ability to enter into new contracts, execute our sales strategy and achieve our expected retention rates include, but are not limited to, the following:
•the price, performance, functionality and security of the Privia Technology Solution;
•Privia Physician and Medical Group adoption of new services;
•our ability to adapt to emerging demands, including adapting to the ways in which providers, patients, payers and other third parties interact with the Privia Technology Solution, the Privia Platform, and our operating model;
•our ability to innovate, develop complementary solutions and evolve our service offerings in a way that is useful to providers, patients and payers;
•our ability to invest in research and development and obtain reasonable returns on such investments;
•the availability, price and performance of competing solutions; and
•industry consolidation.
If contracts are negotiated with lower fee levels or other less favorable terms, if we determine it is necessary to adjust our pricing model, if customers fail to purchase or utilize additional products and services we offer, or if contracts are not renewed, our revenues may decline and future growth may be constrained. If a Medical Group or Privia Provider terminates their relationship with us after implementation has begun, we would lose the resources invested in that relationship and the opportunity to leverage those resources to build relationships with other Privia Providers over the same period of time. If a health system partner that is the majority owner of a Non-Owned Medical Group terminates our partnership or affiliation, we may not be able to identify an alternative partner to
implement the operating model or restructure in a way to retain a sufficient number of Privia Physicians, which may restrict our ability to continue operations in that market. Even if we identify an alternative partner or are otherwise able to continue operations, we may be subject to contractual prohibitions that could adversely affect our ability to operate, such as limitations on our ability to retain Privia Providers in the market, or challenges with transitioning operations that could result in financial or operational impacts that could lead to dissatisfaction among Privia Providers. If we are not able to establish, retain or maintain on favorable terms any of these contractual relationships, our business, operations and financial condition may be adversely impacted.
The success of our business depends on the execution of our growth strategy, which may not prove viable and we may not realize expected results.
Our business strategy is to grow rapidly by increasing Privia Providers in existing markets and acquiring new Medical Groups, ACOs, independent physician associations, and clinically integrated networks in new geographic markets. New market growth is significantly dependent on partnering with anchor medical practices or health systems or hospitals in such new geographic markets. Likewise, our growth strategy is dependent on growing same-store sales for our Medical Groups by offering new services, such as our virtual visit platform or certain ancillary services, assisting our Medical Groups in recruiting new clinicians, and partnering or contracting with commercial payers to enter new VBC arrangements on behalf of our Medical Groups. We seek growth opportunities both organically and through alliances with other parties in the healthcare industry.
Our growth strategy involves a number of risks and uncertainties, including that:
•we and our Medical Groups may not be able to contract with payers on terms favorable to us or at all;
•we and our Medical Groups face competition for payer contracts and this competition may intensify, including as a result of ongoing consolidation in the healthcare industry;
•we may not be able to recruit or retain a sufficient number of new Medical Groups, and we and our Medical Groups may not be able to recruit or retain a sufficient number of Privia Physicians or patients, to execute our growth strategy, or to fully implement our operating model in new markets, and we may incur substantial recruiting and marketing costs;
•we may fail to integrate new Privia Providers or their support staff into our operating model;
•when expanding our business into new markets, compliance with additional laws and regulations may slow our expected growth or limit our potential market of available physicians or the services and solutions we may offer; and
•we may fail to realize expected synergies, financial, strategic or other benefits from same-store sales or expansion into new markets or face challenges successfully integrating new Medical Groups or Privia Providers into our operating model and the Privia Technology Solution.
There can be no assurance that we will be able to successfully capitalize on growth opportunities and otherwise execute our growth strategy, which may negatively impact our business model, revenues, results of operations and financial condition.
We may encounter difficulty acquiring entities or assets, face challenges integrating the operations of acquired businesses or realizing expected results or become liable for unknown or contingent liabilities as a result of acquisitions.
A component of our business strategy is making acquisitions and entering into joint ventures with other parties in the healthcare industry. If we fail to identify and successfully complete transactions to meet our strategic objectives, including as a result of healthcare regulatory or antitrust considerations or actions or as a result of any failure to successfully integrate acquired businesses and realize expected synergies, we may be placed at a competitive disadvantage or be adversely affected by negative market perceptions, any of which may have a material adverse effect on our results of operations, financial position or cash flows. Successful acquisitions also require us to efficiently and effectively integrate the acquired business into our existing operations, including our internal control environment, culture and compliance programs, such as our data security programs. For example, we may experience information technology system vulnerabilities or litigation risks in recently acquired business. We may be unable to address fully or cost-effectively contain such vulnerabilities quickly following the acquisition or at all, which could undermine integration activities or increase risks and costs. In addition, even with appropriate diligence, pre-acquisition practices of an acquired business have exposed us in the past and may expose us in the future to legal challenges and investigations that could subject us to regulatory scrutiny or reputational harm, among other risks. Even if we are ultimately successful in resolving these matters, defending such claims may be costly and result in negative publicity or reputational harm. If we cannot successfully integrate our acquired businesses and realize contemplated revenue growth opportunities, cost savings and other synergies, our business, prospects, results of operations, financial position and cash flows could be materially and adversely affected.
If we fail to manage our growth effectively, we may be unable to execute our business plan, maintain high levels of stakeholder service and patient satisfaction, or adequately address competitive challenges.
We have experienced, and may continue to experience, rapid growth and organizational change, which has placed, and may continue to place, significant demands on our management and our operational and financial resources. We may also seek growth opportunities through strategic acquisitions and partnerships. Additionally, our organizational structure may become more complex as we improve our operational, financial and management controls, as well as our reporting systems and procedures. We may require significant
capital expenditures and the allocation of valuable management resources to grow and change in these areas. We must effectively increase our headcount and continue to effectively train, manage and retain our employees. We will be unable to manage our business effectively if we are unable to alleviate the strain on resources caused by growth in a timely and successful manner. If we fail to effectively manage our anticipated growth, the quality of our services may suffer, which could negatively affect our brand and reputation and harm our ability to attract and retain Medical Groups, Privia Providers, patients and employees. If we fail to evaluate and execute new business opportunities properly, we may not achieve anticipated benefits and may incur increased costs.
In addition, as we expand our business, it is important that we continue to maintain a high level of stakeholder service and satisfaction. As our Privia Physician base continues to grow, we will need to expand our population health, patient services and other personnel, either through employment or contractual arrangements to provide personalized stakeholder service. If our Medical Groups are not able to continue to provide high quality cost effective healthcare services with high levels of patient satisfaction, our reputation, as well as our business, results of operations and financial condition could be adversely affected, including a failure to realize the benefits of any VBC arrangements.
If the estimates and assumptions we use to determine the size of our total addressable market, or TAM, are inaccurate, our future growth rate may be impacted and our business could be harmed.
Market estimates and growth forecasts, including related to the TAM for available physicians with which our Medical Groups can affiliate, are subject to significant uncertainty and are based on assumptions and estimates that may not prove to be accurate. Even if the markets in which we compete meet our size estimates and forecasted growth, our business could fail to grow at similar rates, if at all.
The principal assumptions relating to our determination of the TAM includes determining the total number of physicians in the geographic market reduced by hospital employed physicians and other Privia Physicians in the market that are unlikely to change their existing relationships. This calculation may not take into account physicians who are not currently available because of an exclusive arrangement with an intermediary entity or because the physician is locked out of moving while awaiting payment pursuant to a VBC arrangement. We also evaluate the variation in physician reimbursement by commercial payers in each market to determine if there is a sufficiently large TAM to allow us to affiliate with a sufficiently large number of physicians. We also evaluate the variation in physician reimbursement by commercial payers in each market to determine if there is sufficient economic opportunity to allow physicians to embrace our Privia operating model. Our TAM is also based on the assumption that the strategic approach that our solution enables for potential Privia Physicians will be more attractive to our available physicians than many competing opportunities. If these assumptions prove inaccurate, our business, financial condition and results of operations could be adversely affected.
If certain of our vendors do not meet our needs, if there are material price increases or reductions in reimbursement rates on vendor services and products, if they experience service disruptions as a result of factors outside of our control, or if we are unable to effectively access new or replacement services or products, our business, ability to operate, financial condition, cash flows, results of operations, and relationships with our Medical Groups, Privia Providers and their patients could be negatively impacted.
The ability of the Company and its Medical Groups to offer services and solutions and to maintain business operations is dependent on maintaining relationships with third-party vendors and entering into new relationships to meet changing business needs. Any deterioration in vendor relationships or failure to enter into agreements with vendors in the future could harm our business and our ability to pursue our growth strategy. If any third-party vendors of the Company, its Medical Groups, or ACOs are unable or unwilling (including as a result of a product recall, shortage, dispute or cybersecurity incident) to provide the services necessary to support our business, if our vendors do not meet our needs for the services or products they supply (including as a result of vendors updating or replacing services and products), if we experience material price increases from vendors or reductions in reimbursement rates that we are unable to mitigate, if we are not able to access new or replacement services on a cost-effective basis or at all, or if vendors are unable to scale as fast as our operations grow or provide services required to meet the changing needs of our business, it could have a material adverse effect on our operations. We, our Medical Groups, and ACOs may incur substantial costs, delays and disruptions to our business in transitioning such services to internal platforms or other third-party vendors. Any of the foregoing could materially harm our competitive position, business, results of operations, financial condition and cash flows. We, our Medical Groups, and ACOs have vendors that may be the sole or primary source of certain services, products or technology critical to the services either we, our Medical Groups, Privia Providers, or ACOs furnish, which augments the aforementioned risks with respect to these vendors.
For example, we are dependent on our EMR vendor, athenahealth, Inc., with which the Privia Technology Solution is integrated, and which is utilized by most of our Medical Groups. Our business could be adversely affected if that relationship were disrupted. The Privia Technology Solution may be less effective with other EMRs, and moving Privia Providers to another EMR provider would require considerable effort, time and expense. In addition, our dependency and the dependency of most of our Medical Groups on athenahealth, Inc., heightens risks related to service disruptions or potential cybersecurity incidents experienced by, cessation of operations of, future price increases by, or privacy (including HIPAA) and AI regulation compliance by this vendor. Furthermore, changes to the athenahealth, Inc. platform could require us, our Medical Groups or Privia Providers to make financial or operational investments or changes to respond to such changes to the platform. A material change in our relationship with athenahealth, Inc., whether resulting from a dispute, a change in government regulation, other factor or the loss of this relationship, could impair our ability to provide services to Privia Providers, could impact our approach to regulatory compliance, and could have a materially
adverse effect our business, financial condition and results of operations. Additionally, certain of the Company’s service providers, including technology or AI-related service providers, may experience service disruptions from a variety of factors outside of the Company’s control ranging from severe or extreme weather to cybersecurity incidents and geopolitical conflict, and our operations could be negatively impacted by any disruption or vulnerabilities in the services they provide resulting from such factors outside our control.
If we are not able to maintain and enhance our reputation and brand recognition, including through the maintenance and protection of trademarks, our business and results of operations will be harmed.
We believe that maintaining and enhancing our reputation and brand recognition is critical to our relationships with Medical Groups, Privia Providers, patients, ACO participants, and payers, and to our ability to attract new Medical Groups, Privia Physicians, ACO participants, and patients. The promotion of our brand may require us to make substantial investments and we anticipate that, as our market becomes increasingly competitive, these marketing initiatives may become increasingly difficult and expensive. Our marketing activities may not be successful or yield increased revenue, and to the extent that these activities yield increased revenue, the increased revenue may not offset the expenses we incur and our results of operations could be harmed. In addition, any factor that diminishes our reputation or that of our management, including failing to meet the expectations of our Medical Groups, Privia Physicians, ACO participants, health system or hospital partners, patients, or payers, or any adverse publicity or litigation involving or surrounding us, any of our Medical Groups, Privia Providers or our management, could make it substantially more difficult for us to attract new Privia Physicians, New Medical Group, or retain existing Privia Providers and Medical Groups. Similarly, because our existing Medical Groups often act as references for us with prospective Privia Physicians or new Medical Groups, any reputational concerns could impair our ability to secure additional new Privia Physicians and Medical Groups. In addition, negative publicity resulting from any adverse government investigation or payer audit could injure our reputation. If we do not successfully maintain and enhance our reputation and brand recognition, our business may not grow and we could lose our relationships with Privia Physicians, Medical Groups, ACO participants, health system or hospital partners, patients, or payers, which could harm our business, results of operations and financial condition.
The registered or unregistered trademarks or trade names that we own or license may be challenged, infringed, circumvented, declared generic, lapsed or determined to be infringing on or dilutive of other marks. We may not be able to protect our rights in these trademarks and trade names, which we need in order to build name recognition with patients, payers and other third parties. In addition, third parties may in the future file for registration of trademarks similar or identical to our trademarks. If they succeed in registering or developing common law rights in such trademarks, and if we are not successful in challenging such third-party rights, we may not be able to use these trademarks to commercialize our technologies in certain relevant jurisdictions. If we are unable to establish name recognition based on our trademarks and trade names, we may not be able to compete effectively and our brand recognition, reputation and results of operations may be adversely affected.
The operations of the Company and its Medical Groups are concentrated in certain U.S. states in which we have a presence, which makes us sensitive to regulatory, economic, public health, environmental, competitive and other conditions and changes in these jurisdictions, and we may not be able to successfully establish a presence in new geographic markets.
A substantial portion of our revenue is driven by our Medical Groups and ACOs in certain U.S. states, in which we have a presence. As a result, our exposure to many of the risks described herein are not mitigated by a diversification of geographic focus. Furthermore, the concentration of the operations of the Company and its Medical Groups makes our business particularly sensitive to regulatory, economic, environmental (including natural disasters), competitive and other conditions and changes in these jurisdictions. Any material change in payment programs or regulatory, economic, public health, environmental or competitive conditions in these states or the District of Columbia could have a disproportionate effect on our operating results and financial condition, and could disrupt the operations of our Medical Groups, Privia Providers, and ACOs. The risks of geographic concentration could decrease as we expand the operations of the Company and its Medical Groups to other regions of the United States, but expansion is resource-intensive and we may encounter significant barriers to entry in new markets. We anticipate that further geographic expansion may require us to make a substantial investment of management time, capital and/or other resources. There can be no assurance that we will be able to continue to successfully expand our operations in any new geographic markets.
Changes in treatment methodologies, trends related to the usage of primary care and specialist healthcare services, and other factors outside our control that impact demand for medical services may reduce our revenues.
Patient volumes and case-mix trends related to the usage of primary care and specialist healthcare services may be impacted by factors beyond the control of the Company and its Medical Groups, such as changes in volume of certain high acuity services, variations in the prevalence and severity of outbreaks of influenza, COVID-19 and other illnesses, seasonal and severe weather conditions, changes in treatment regimens and medical technology and other advances. Further, trends in physician treatment protocols and health plan design, such as health plans that shift increased costs and accountability for care to patients, could reduce the volume of certain procedures and treatments rendered by Privia Providers in favor of lower intensity and lower cost treatment methodologies or result in patients seeking care from other providers or failing to obtain appropriate, medically necessary care. These and other factors beyond the control of the Company and its Medical Groups may reduce the demand for services we offer and decrease the reimbursement that we receive, which could have a material, adverse effect on our business, financial position, and results of operations.
The failure to obtain medical supplies, drugs and other goods for Medical Groups at favorable prices or in sufficient volumes could cause our results of operations to decline.
Costs of medical supplies, drugs and other goods may continue to increase due to market pressure from pharmaceutical companies and vendors, new product releases, product shortages and other factors including import/export restrictions, such as new, expanded or retaliatory tariffs, sanctions, quotas or trade barriers (including recently-imposed U.S. tariffs and any reciprocal tariffs or similar actions taken by target countries). If we or our Medical Groups are unable to obtain sufficient supplies or are unable to access new or replacement products, it could negatively impact the ability of our Medical Groups to provide services to patients. Higher costs and insufficient supplies could adversely affect our business, results of operations, financial condition, and cash flows.
Technology, Cybersecurity and Privacy Risks
Security threats, cybersecurity incidents or other forms of data breaches, catastrophic events and other disruptions to our, our Medical Groups’ and ACOs’, our business partners’ or our vendors’ information technology and related systems could compromise sensitive information related to our business, the Medical Groups or patients, prevent access to critical information, harm patients, require remediation and other corrective action, which can be expensive, and expose us to liability, which could adversely affect our business, operations and reputation.
Information technology is a critical component of the day-to-day business operations of the Company, its Medical Groups, and ACOs. Our business is highly dependent on maintaining effective information systems, in part because VBC arrangements involve extensive data processing and analytics, as well as the integrity and timeliness of the data we use to serve our Privia Providers’ patients, support our Medical Groups and Privia Providers, monitor and manage our ACOs and management services organizations (including satisfaction of reporting obligations) and to otherwise operate our business. We, our Medical Groups, and ACOs, directly and through our vendors and other third parties, collect and store on networks, devices and third-party technology platforms sensitive information, including intellectual property, proprietary and confidential business information, protected health information of patients and personally identifiable information of our employees and patients. Our Medical Groups use EMRs and medical devices that are integral to the provision of patient care, and these systems and devices are increasingly connected to the internet and other downstream technology platforms. We have implemented multiple layers of security measures to protect the confidentiality, integrity and availability of our data, networks, systems and devices. Our and the Medical Groups’, and ACOs’ systems interface with and rely on third-party provided systems that we do not directly control, such as the athenahealth EMR and platforms that support the interoperability of the healthcare infrastructure for treatment, payment and operations. Third-party technology platforms are increasingly important to our business and continue to grow in complexity and scope. We rely on third-party providers to have appropriate controls (including with respect to their own downstream third-party vendors) that protect confidential information and other sensitive or regulated data that is on their systems or otherwise in their control. Our contracts with such third-party providers typically include terms holding them to our security standards.
We, our Medical Groups and our vendors have been and continue to be the target of attempted cybersecurity and other threats that could have a security impact, including efforts by third parties, including threat actors, to access, misappropriate, corrupt or manipulate our information or disrupt our operations. Despite our implementation of security measures, we expect to continue to experience an increase in cybersecurity threats in the future, as the volume, intensity and sophistication of cyberattacks continue to increase, particularly within the healthcare industry. Threats from malicious persons and groups, new vulnerabilities and advanced new attacks against our, our Medical Groups’, Privia Providers’ medical practices’, or our vendors’ information systems and devices create risk of cybersecurity incidents, including ransomware, data exfiltration, malware and phishing incidents as well as social engineering attacks, including AI-enabled social engineering attacks. As cybersecurity threats continue to evolve, we and our Medical Groups may not anticipate certain techniques used to obtain unauthorized access to, or to sabotage, information systems, and we may not be able to implement effective protective measures. We and our Medical Groups may experience security incidents that remain undetected for an extended period, or, even if identified, we may be unable to adequately investigate or remediate incidents or breaches due to attackers using tools and techniques designed to circumvent controls, avoid detection, and remove or obfuscate forensic evidence. The rapid evolution and increased adoption of AI technologies may intensify our cybersecurity risks. Moreover, hardware, software or applications that we, our Medical Groups and vendors use may have inherent vulnerabilities or defects of design, manufacture or operations or could be inadvertently or intentionally implemented or used in a manner that could compromise information security.
As cyber threats continue to evolve and the volume and sophistication of threats increases, we may be required to expend significant additional resources to continue to modify or enhance security measures and investigate and remediate any potential vulnerabilities in our information technology systems and infrastructure. Although to date no cyberattack or other information or security breach has resulted in material losses or other material consequences to us, there can be no assurance that our controls and procedures in place to monitor and mitigate the risks of cyber threats will be sufficient and/or timely. We, our Medical Groups, ACOs, or our vendors could be subject to incidents that bypass security measures, impact the integrity, availability or privacy of PHI or other data subject to privacy laws or disrupt our or their information systems, devices or business, including the ability to provide various healthcare services. In such an event, we or our Medical Groups may incur substantial costs, including but not limited to, costs associated with remediating the effects of the cybersecurity incident, costs for security measures to guard against similar future incidents and costs to recover data. In addition, the occurrence of cybersecurity incidents or other forms of data breaches or disruptions could result in harm
to patients; business interruptions and delays; the loss, misappropriation, corruption or unauthorized access of data; litigation and potential liability under privacy, security, breach notification and consumer protection laws (including penalties imposed under HIPAA), common law theories or other applicable laws; reputational damage; and foreign, federal and state governmental inquiries, any of which could have a material, adverse effect on our financial position and results of operations and harm our business relationships and reputation. While we, our Medical Groups, and ACOs have in place insurance coverage designed to address certain aspects of cyber risks, such insurance coverage may be insufficient to cover all losses or all types of claims that may arise. Further, to the extent there are successful cyberattacks at other healthcare services companies, consumer confidence in the integrity and security of personal information and critical operations data in the healthcare industry generally could be shaken, which could have a material, adverse effect on our business, financial position or results of operations.
In addition to the risk of cyber threats, information systems may be vulnerable to damage from a variety of other sources, including telecommunications or network failures, human acts such as inadvertent or intentional misuse by employees or contractors and natural disasters. Despite precautionary measures, we, our Medical Groups, ACOs, or our vendors and other third-parties (or their downstream third-party vendors) that we rely upon may experience system failures and disruptions. Although we have disaster recovery systems and business continuity plans in place, we cannot provide assurance that there will not be disruptions in or other failures of our disaster recovery systems, and we cannot provide assurance that our business continuity plans sufficiently protect against extended technology or service outages of our third-parties. For example, certain of our vendors may utilize a limited number of regional data centers and any disruption at such a data center could cause widespread disruption to our business. The occurrence of any such or similar system failure could result in interruptions, delays, the loss or corruption of data and cessations or interruptions in the availability of systems, any of which could have a material, adverse effect on patient care, our financial position and results of operations and lead to reputational harm.
If we or our Medical Groups experience failures or interruption in services we receive through third-party internet infrastructure, bandwidth providers, EMR and other vendors, our business, ability to operate, financial condition, cash flows, results of operations, and relationships with our Medical Groups, Privia Providers and their patients could be negatively impacted.
The Company and its Medical Groups rely on internal systems as well as third-party suppliers, including network and infrastructure equipment providers, to maintain the Privia Platform, the Privia Technology Solution and related services. Failure to adequately manage updates or enhancements to such platforms or interfaces between platforms or implementation of new technology could place us at a competitive disadvantage, disrupt operations and have a material, adverse impact on our business and results of operations. Further, our ability to maintain the Privia Technology Solution, including our virtual health services, is dependent on the development and maintenance of the infrastructure of the internet (including a reliable network connection with the necessary speed, data capacity and security for providing reliable internet access and services), reliable telephone and facsimile services and other services furnished by third parties. Although we maintain redundancy with respect to the critical components of our platform, we do not currently maintain redundant systems or facilities for some of the services on which we depend. The Privia Technology Solution is designed to operate without perceptible interruption in accordance with our service level commitments.
We have, however, experienced limited interruptions in these systems in the past, including temporary slowdowns in the performance of our EMR and the Privia Technology Solution, and we may experience similar or more significant interruptions in the future.
Interruptions in third-party systems or services, or our own or our Medical Groups’ systems, whether due to system failures, cyber incidents, physical or electronic break-ins or other events, could affect the security or availability of the Privia Platform and Medical Group services, including EMR access, patient scheduling, patient and Privia Physician portals; prevent or limit access to the Privia Technology Solution or other services by Privia Providers and their patients; result in noncompliance with privacy laws and regulations; result in the loss of proprietary or personal information; hurt our relationships with Medical Groups, Privia Physicians, patients, payers, and other network participants; and expose us and our Medical Groups to third-party liabilities. In the event of a catastrophic event with respect to one or more of these systems or facilities, we and our Medical Groups may experience an extended period of system unavailability, which could result in substantial remediation costs and harm our business relationships and our business. Any interruption or delay in third-party systems and services could harm our competitive position, business, financial condition, results of operations and prospects.
We and our Medical Groups take steps to monitor the performance of third-party vendors, including in our agreements with such parties, but our oversight controls could prove inadequate. Since we do not fully control the actions of vendors and other third parties, including our Medical Groups and Privia Providers, we are subject to the risk that their decisions or operations could adversely impact us and our Medical Groups, and replacing such third-party vendors could create significant delay and expense. If these third-party vendors fail to satisfy their obligations to us or our Medical Groups, timely comply with legal or regulatory requirements, or deliver high-quality services, the operations and reputation of the Company and its Medical Groups could be compromised, we may not realize the anticipated economic and other benefits from these arrangements, and we could suffer adverse legal, regulatory and financial consequences. In addition, these third parties face their own technology, operating, business and economic risks, and any significant failures by them, including the improper use or disclosure of confidential Company or Medical Group information or failure to comply with applicable laws and regulations, or any failure by them to effectively oversee, monitor or protect against their own downstream third-party vendors’ risks (so-called “fourth-party risk”), could result in reputational harm or otherwise expose the Company and its Medical Groups to liability.
For additional risks related to our third-party vendors, see “If certain of our vendors do not meet our needs, if there are material price increases or reductions in reimbursement rates on vendor services and products, if they experience service disruptions as a result of factors outside of our control, or if we are unable to effectively access new or replacement services or products, our business, ability to operate, financial condition, cash flows, results of operations, and relationships with our Medical Groups, Privia Providers and their patients could be negatively impacted.”
If we cannot timely implement the Privia Technology Solution for Privia Physicians and new Medical Groups, or promptly resolve Privia Provider and patient concerns, or if the Privia Technology Solution fails to operate as we expect, our business and results of operations may be adversely impacted, we could be subject to litigation, and our reputation may be harmed.
The Privia Technology Solution, our end-to-end, cloud-based technology-enabled platform, provides patients with the ability to schedule services with our Privia Physicians and communicate and interact with providers, and it allows our Privia Providers to streamline patient charting and identify gaps in care and conduct virtual visits (via video, phone or the internet), among other functions. The seamless onboarding of Privia Physicians onto the Privia Technology Solution, including training on conversion to and the use of our EMR and the credentialing of Privia Physicians and other providers with applicable federal health care programs and commercial payers is essential to a timely transition to the Privia Technology Solution. As of December 31, 2025, practices on the Privia Technology Solution were converted from approximately 50 different EMR vendors. If we face unanticipated implementation difficulties or Medical Groups, Privia Physicians or support staff are unable or unwilling to smoothly transition to the Privia Technology Solution, we risk delaying the go live date of our new Medical Groups. Delays could cause us to incur significant costs and negatively impact our revenue, and Privia Providers could become dissatisfied, which could negatively impact our reputation, our relationships with Privia Providers, our ability to attract and retain new providers or our ability to negotiate and perform in payer contracts.
We also face risks related to the operation of the Privia Platform and the Privia Technology Solution. Proprietary software development is time-consuming, expensive and complex, and may involve unforeseen difficulties. We may encounter technical obstacles, and it is possible that we may discover additional problems that prevent our proprietary software from operating properly. We are currently implementing software for a number of new applications and services. If our solutions do not function reliably or fail to satisfy user expectations, we may lose or fail to grow our Medical Groups, Privia Provider relationships and patient volumes, we or our Medical Groups could face liability claims, and our Medical Groups, affiliate providers, health system partners, and ACO participants may attempt to terminate their relationships with us. This could damage our reputation and impair our ability to attract or maintain Medical Groups, Privia Providers, patients and relationships with commercial payers.
Medical Groups, Privia Providers and their patients depend on our call center support services to resolve their operational concerns including technical issues relating to the Privia Technology Solution and services and patient billing inquiries. It is difficult to predict demand for call center support services, and if demand increases significantly, we may be unable to provide satisfactory support services in the short- and long-term to our Privia Physicians and their patients, particularly as we increase the size of our Privia Physicians and patient bases. We also may be unable to modify the format of our support services to compete with changes in support services provided by competitors. If we are unable to address our Privia Physicians and their patients’ needs in a timely fashion or further develop and enhance our support services, or if a Privia Physician or patient is not satisfied with the quality of work performed by us or with the call center support services rendered, then we could incur additional costs to address the situation. In addition, our profitability may be impaired and our Privia Physicians and their patients’ dissatisfaction with our support services could damage our ability to retain Medical Groups, Privia Physicians and their patients. Such Medical Groups or Privia Physicians may not renew their contracts, seek to terminate their relationship with us or renew on less favorable terms. Moreover, negative publicity related to our Medical Groups and Privia Physician relationships, regardless of its accuracy, may further damage our business by affecting our reputation or ability to compete for new Privia Physicians in the market. If any of these were to occur, our revenue may decline and our business, financial condition and results of operations could be adversely affected.
Our business depends on our ability to effectively invest in, implement improvements to and properly maintain our information technology and other business systems.
Our information technology strategy and execution are critical to our continued success. We must continue to invest in long-term solutions that will enable us to anticipate our Medical Groups, Privia Providers, ACOs, and commercial payers’ needs and expectations, enhance both Privia Providers’ and patients’ experience, act as a differentiator in the market and protect against cybersecurity risks and threats. Our success is dependent, in large part, on maintaining the effectiveness of existing technology systems, including using systems and tools provided by third-party vendors and continuing to deliver and enhance technology systems that support our business processes in a cost-efficient and resource-efficient manner. Increasing regulatory and legislative changes may place additional demands on our information technology infrastructure, which could impact availability of resources for other projects tied to our strategic initiatives. In addition, recent trends toward greater patient engagement in health care require new and enhanced technologies, including more sophisticated applications for mobile devices. Connectivity among technologies is becoming increasingly important. We must also develop new systems to meet current market standards and keep pace with continuing changes in information processing technology, evolving industry and regulatory standards and patient needs, while protecting against evolving cybersecurity threats. Failure to do so may present compliance challenges and impede our ability to deliver services in a competitive manner or expose our technology and business systems to cybersecurity risks. Further, because system development projects are long-
term in nature, they may be more costly than expected to complete and may not deliver the expected benefits upon completion. Our failure to effectively invest in, implement improvements to and properly maintain the uninterrupted operation and data integrity of our information technology and other business systems could adversely affect our results of operations, financial position and cash flow.
If we are unable to obtain, maintain and enforce intellectual property protection for our technology or if the scope of our intellectual property protection is not sufficiently broad, others may be able to develop and commercialize technology substantially similar to ours, and our ability to successfully commercialize our technology may be adversely affected.
Our business depends, in part, on internally developed technology and content, including software, databases, confidential information and know-how, the protection of which is crucial to the success of our business. We rely on a combination of trademark, trade-secret, and copyright laws and confidentiality procedures and contractual provisions to protect our intellectual property rights in our internally developed technology and content and our brand. We may, over time, increase our investment in protecting our intellectual property through additional trademark, patent and other intellectual property filings that could be expensive and time-consuming to develop and maintain, both in terms of initial preparation and ongoing registration requirements and the costs of defending our rights. These measures, and the steps we have taken to protect our intellectual property rights may not be adequate to prevent infringement, misappropriation or other violations of our intellectual property. If we are unable to establish or protect our intellectual property and other rights, our competitive position and our business could be harmed, as third parties may be able to commercialize and use technologies and software products that are substantially the same as ours without incurring the development and licensing costs that we have incurred. Any of our owned or licensed intellectual property rights could be challenged, invalidated, circumvented, infringed or misappropriated, our trade secrets and other confidential information could be disclosed in an unauthorized manner to third parties, or our intellectual property rights may not be sufficient to permit us to take advantage of current market trends or otherwise to provide us with competitive advantages, which could result in costly redesign efforts, discontinuance of certain offerings or other competitive harm.
Uncertainty may result from changes to intellectual property legislation and from interpretations of intellectual property laws by applicable courts and agencies. In addition, advances in AI technology may exacerbate these risks, including the risk that existing intellectual property laws may not adequately protect against advances in AI technology, giving rise to a proliferation of infringement which we may not be able to address effectively; the risk that the use of generative AI tools could result in us inadvertently disclosing trade secrets or other confidential information; and the risk that the use of generative AI in the creation of our source code may not be protectable under existing intellectual property laws. Accordingly, despite our efforts, we may be unable to obtain and maintain the intellectual property rights necessary to provide us with a competitive advantage. Our failure to obtain, maintain and enforce our intellectual property rights could therefore have a material adverse effect on our business, financial condition and results of operations.
Third parties may allege that we are infringing, misappropriating or otherwise violating their intellectual property rights and in some instances initiate formal legal proceedings, the outcome of which would be uncertain and could have a material adverse effect on our business, financial condition and results of operations.
Our commercial success depends on our ability to develop, commercialize and protect the Privia Platform, the Privia Technology Solution and the Privia operating model, and use our internally developed technology without infringing, misappropriating or otherwise violating the intellectual property or proprietary rights of third parties. Intellectual property disputes can be costly to defend, may divert management’s attention or resources and may cause our business, operating results and financial condition to suffer. As the market for healthcare in the United States expands and more patents are issued, the risk increases that there may be patents issued to third parties that relate to our technology of which we are not aware or that we must challenge to continue our operations as currently contemplated. Whether merited or not, we may face allegations that we, our partners or parties indemnified by us have infringed, misappropriated or otherwise violated the patents, trademarks, copyrights or other intellectual property rights of third parties. Such claims may be made by competitors seeking to obtain a competitive advantage or by other parties. Additionally, in recent years, individuals and groups have begun acquiring intellectual property assets for the purpose of making claims of infringement and attempting to extract settlements from companies like ours. We may also face allegations that our employees have misappropriated the intellectual property or proprietary rights of their former employers or other third parties. It may be necessary for us to initiate litigation to defend ourselves in order to determine the scope, enforceability and validity of third-party intellectual property or proprietary rights, or to establish or enforce our respective rights. We may not be able to successfully settle or otherwise resolve such adversarial proceedings or litigation. If we are unable to successfully settle future claims on terms acceptable to us, we may be required to defend such claims, regardless of their underlying merit, that can be time-consuming, divert management’s attention and financial resources and can be costly to evaluate and defend. Results of any such litigation are difficult to predict and may require us to stop commercializing or using our technology, obtain licenses, modify our services and technology while we develop non-infringing substitutes or incur substantial damages, settlement costs or face a temporary or permanent injunction prohibiting us from marketing or providing the affected services. If we require a third-party license, it may not be available on reasonable terms or at all, and we may have to pay substantial royalties, upfront fees or grant cross-licenses to intellectual property rights for our services. We may also have to redesign our services so they do not infringe, misappropriate or violate third-party intellectual property rights, which may not be possible or may require substantial monetary expenditures and time, during which our technology may not be available for commercialization or use. Even if we have an agreement to indemnify us against such costs, the indemnifying party may be unable to uphold its contractual obligations. If we cannot or do not obtain a third-party license to the infringed technology at all, license the
technology on reasonable terms or obtain similar technology from another source, our revenue and earnings could be adversely impacted.
Some third parties may be able to sustain the costs of complex litigation more effectively than we can because they have substantially greater resources. Even if resolved in our favor, litigation or other legal proceedings relating to intellectual property claims may cause us to incur significant expenses, and could divert our technical personnel and management’s attention from the operation of our business. In addition, there could be public announcements of the results of hearings, motions or other interim proceedings or developments, and if securities analysts or investors perceive these results to be negative, it could have a material adverse effect on the price of our common stock. Assertions by third parties that we infringe, misappropriate or otherwise violate their intellectual property rights could therefore have a material adverse effect on our business, financial condition and results of operations.
If we are unable to protect the confidentiality of our trade secrets, know-how and other proprietary and internally developed information, the value of our technology could be adversely affected.
We may not be able to protect our trade secrets, know-how and other internally developed information adequately. Although we use reasonable efforts to protect this internally developed information and technology, our employees, consultants, Privia Providers and other parties (including independent contractors and companies with which we conduct business) may unintentionally or willfully disclose our information or technology to competitors. Enforcing a claim that a third-party illegally disclosed or obtained and is using any of our internally developed information or technology is difficult, expensive and time-consuming, and the outcome is unpredictable. In addition, courts outside the United States are sometimes less willing to protect trade secrets, know-how and other proprietary information and the laws regarding such protections vary among jurisdictions. We rely, in part, on non-disclosure, confidentiality and assignment-of-invention agreements with our employees, independent contractors, and consultants with which we conduct business to protect our trade secrets, know-how and other intellectual property and internally developed information. However, we may fail to enter into such agreements with all of our employees, independent contractors, consultants, customers and other companies, and these agreements may not be self-executing, or they may be breached and we may not have adequate remedies for such breach. Moreover, third parties may independently develop similar or equivalent proprietary information or otherwise gain access to our trade secrets, know-how and other internally developed information and the value of our technology could be adversely impacted.
Any restrictions on our use of, or ability to license, data, or our failure to license data and integrate third-party technologies, could have a material adverse effect on our business, financial condition and results of operations.
We depend upon licenses from third parties for some of the technology and data used in the Privia Technology Solution and the Privia Platform. We expect that we may need to obtain additional licenses from third parties in the future in connection with the development of our services. In addition, we obtain a portion of the data that we use from government entities, public records and from third parties for specific engagement and uses. We believe that we have all rights necessary to use the data that is incorporated into our services. We cannot, however, make assurances that our licenses for information will allow us to use that information for all potential or contemplated applications. In addition, our ability to continue to offer integrated healthcare to our patients depends on maintaining the Privia Technology Solution, which is partially populated with data disclosed to us by our partners with their consent. If these partners revoke their consent for us to maintain, use, de-identify and share this data, consistent with applicable law, our data assets could be degraded.
In the future, data providers could withdraw their data from us or restrict our usage for any reason, including if there is a competitive reason to do so, if legislation is passed restricting the use of the data or if judicial interpretations are issued restricting use of the data that we currently use to support our services. In addition, data providers could fail to adhere to our quality control standards in the future, causing us to incur additional expense to appropriately utilize the data. If a substantial number of data providers were to withdraw or restrict their data, or if they fail to adhere to our quality control standards, and if we are unable to identify and contract with suitable alternative data suppliers and integrate these data sources into our service offerings, our ability to provide appropriate services to our Privia Providers, Medical Groups, health system or hospital partners, patients, and commercial payer customers could be materially adversely impacted, which could have a material adverse effect on our business, financial condition and results of operations.
We also integrate into our internally developed applications and use third-party software to support our technology infrastructure. Some of this software is proprietary and some is open source software. These technologies may not be available to us in the future on commercially reasonable terms or at all and could be difficult to replace once integrated into our own internally developed applications. Most of these licenses can be renewed only by mutual consent and may be terminated if we breach the terms of the license and fail to cure the breach within a specified period. Our inability to obtain, maintain or comply with any of these licenses could delay development until equivalent technology can be identified, licensed and integrated, which could harm our business, financial condition and results of operations.
Most of our third-party licenses are non-exclusive and our competitors may obtain the right to use any of the technology covered by these licenses to compete directly with us. Our use of third-party technologies exposes us to increased risks, including, but not limited to, risks associated with the integration of new technology into our solutions, the diversion of our resources from development of our own internally developed technology and our inability to generate revenue from licensed technology sufficient to offset associated
acquisition and maintenance costs. In addition, if our data suppliers choose to discontinue support of the licensed technology in the future, we might not be able to modify or adapt our own solutions.
Our use of “open source” software could adversely affect our ability to offer our services and subject us to possible litigation.
We use open source software in connection with the Privia Technology Solution. Companies that incorporate open source software into their technologies have, from time to time, faced claims challenging the use of open source software and/or compliance with open source license terms. As a result, we could be subject to suits by parties claiming ownership of what we believe to be open source software or claiming noncompliance with open source licensing terms. Some open source software licenses require users who use software containing open source software to publicly disclose all or part of the source code to such software and/or make available any derivative works of the open source code, which could include valuable proprietary code of the user, on unfavorable terms or at no cost. While we monitor the use of open source software and try to ensure that none is used in a manner that would require us to disclose our internally developed source code or that would otherwise breach the terms of an open source agreement, such use could inadvertently occur, in part because open source license terms are often ambiguous. Any requirement to disclose our internally developed source code or pay damages for breach of contract could have a material adverse effect on our business, financial condition and results of operations and could help our competitors develop services that are similar to or better than ours.
If an author or other third-party that distributes such open source software were to allege that we had not complied with the conditions of one or more of these licenses, we could be required to incur significant legal expenses defending against such allegations and could be subject to significant damages, enjoined from the commercialization of our services that contained the open source software, engaged in costly redesign efforts, and required to comply with onerous conditions or restrictions on these services, which could disrupt the distribution of services. From time to time, there have been claims challenging the ownership rights in open source software against companies that incorporate it into their products and the licensors of such open source software provide no warranties or indemnities with respect to such claims. As a result, we could be subject to lawsuits by parties claiming ownership of what we believe to be open source software. Litigation could be costly for us to defend, have a negative effect on our business, financial condition, cash flows, and results of operations, or require us to devote additional research and development resources to change our services. Some open source projects have known vulnerabilities and architectural instabilities and are provided on an “as-is” basis, which, if not properly addressed, could negatively affect the performance of our platform. If we inappropriately use or incorporate open source software subject to certain types of open source licenses that challenge the proprietary nature of the Privia Technology Solution, we may be required to re-engineer the Privia Technology Solution, discontinue the commercialization of the Privia Technology Solution or take other remedial actions, any of which could adversely impact our business, financial condition, cash flows, and results of operations.
We face risks associated with healthcare technology initiatives, including those related to sharing patient data and interoperability, as well as our use of certain AI and machine learning models.
The federal government is working to promote the adoption of health information technology to improve healthcare, including through the nationwide health information network exchange. As the health information technologies have become widespread, the focus has shifted to increasing patient access to health care data and interoperability. For example, the 21st Century Cures Act and its implementing regulations promote information sharing by prohibiting information blocking by healthcare providers and certain other entities. Information blocking is defined as engaging in activities likely to interfere with the access, exchange or use of electronic health information, except as required by law or specified by HHS as a reasonable and necessary activity. In addition, HHS incentivizes the adoption and meaningful use of certified EMR technology through its Promoting Interoperability Programs. In a final rule published in July 2024, MIPS-eligible clinicians (including group practices, like our Medical Groups) that commit information blocking will not be considered meaningful EMR users during the calendar year for the performance period in which OIG refers its determination to CMS, resulting in a zero score in the MIPS Promoting Interoperability category, which would negatively affect reimbursement. Under the same rule, a provider that is an ACO, ACO participant, or ACO provider or supplier that commits information blocking may be ineligible to participate in MSSP for a period of at least one year.
Our business utilizes, and may invest in the future in, AI, predictive analytics and other AI technologies to add AI-based applications to our offering to drive efficiencies in our business, offer new applications, upgrade our solutions and security, and enhance our capabilities. In addition, certain of our third-party vendors utilize AI in furnishing products and services to us and our Medical Groups and ACOs. These efforts, including the design and introduction of new products and services or changes to existing products and services, may result in new or enhanced governmental or regulatory scrutiny, litigation, ethical concerns, or other complications that could adversely affect our business, reputation, or financial results. Further, information systems, AI and other predictive analytics are susceptible to flaws, biases, malfunctions or manipulations, which may disrupt our and our Medical Groups’ operations, result in erroneous decision-making, elevate our and our Medical Groups’ cyber risk profile, or expose us to liability. Current and future initiatives related to health care technology (including AI and other predictive algorithms), data sharing and interoperability may require changes to the operations of the Company and its Medical Groups, impose new and complex regulatory and compliance obligations and require potentially significant investments in infrastructure. For example, HHS finalized a rule in December 2023 imposing transparency requirements for AI and other predictive algorithms that are part of certified health information technology. Federal and state legislative and regulatory bodies, including at the executive level, continue to signal increased scrutiny and potential rulemaking surrounding the creation, adoption, and leveraging of AI-based or AI-enhanced tools, systems, and functions. The
Company, its Medical Groups, and ACOs may be subject to financial penalties or other disincentives or experience reputational damage for failure to comply with applicable laws and regulations. Changes to existing regulations, their interpretation or implementation or new regulations could impede our use of AI and also may increase our estimated costs in this area. Further, if we are not successful in our efforts to innovate, the performance of our various products, services, and business, as well as our reputation, could suffer or we could incur liability through the violation of laws or contracts to which we are a party. Any of these factors could adversely affect our business, financial condition, and results of operations.
The AI field is complex and rapidly evolving, and we face significant competition from other companies in our industry. Our efforts in developing and deploying AI may not succeed and our competitors may be able to deploy the technology faster. We may further be exposed to competitive risks related to the adoption and application of new technologies by established market participants or new entrants, and others, and market acceptance of AI is uncertain. The speed of technological development may prove disruptive to some of our markets if we are unable to maintain the pace of innovation. Further, professionals specializing in development, deployment, and enterprise adoption of AI represent a niche pool of qualified individuals. Other participants in our market may be more effectively equipped in terms of financial position and underlying technological resources to recruit and/or retain such individuals. To compete effectively we must also be responsive to technological change, potential regulatory developments, and public scrutiny.
Our use, disclosure, and other processing of personal information, including health-related information, is subject to HIPAA, other federal and state privacy and security regulations, and contractual obligations, and our actual or perceived failure to comply with those regulations or contractual obligations could result in significant liability or reputational harm and, in turn, a material adverse effect on our patient base and revenue.
As discussed above under “We conduct business in a heavily regulated industry, which increases our costs and could restrict the conduct of our business, and if the Company or our Medical Groups fail to comply with the extensive applicable healthcare laws and government regulations, which may change from time to time, we could suffer penalties, be required to make significant changes to our operations, or experience reputational harm, any or all of which may adversely affect our business”, numerous state and federal laws and regulations govern the collection, dissemination, use, privacy, confidentiality, security, availability, integrity, and other processing of PHI and personal information, including HIPAA.
HIPAA requires covered entities, like us, our Medical Groups, ACOs, and their business associates to develop and maintain policies and procedures with respect to PHI that is used or disclosed, including the adoption of administrative, physical and technical safeguards to protect such information. Our Medical Groups may be all participants in an “Affiliated Covered Entity” or an “Organized Health Care Arrangement” under HIPAA, which groups legally separate covered entities that consider themselves a single covered entity due to affiliation, some common control or ownership, or through clinical integration and/or care coordination. Participation in an affiliated covered entity or an organized health care arrangement allows us to share certain HIPAA compliance efforts but also provides for joint and several liability for HIPAA violations among all the participants in the Affiliated Covered Entity. In addition to our status as a covered entity, our management services organizations and ACOs may also be “business associates” to our Medical Groups and ACO participants.
Entities that are found to be in violation of HIPAA as the result of a breach of unsecured PHI, a complaint about privacy practices or an audit by the U.S. Department of Health and Human Services (“HHS”), may be subject to significant civil, criminal and administrative fines and penalties and/or additional reporting and oversight obligations if required to enter into a resolution agreement and corrective action plan with HHS to settle allegations of HIPAA non-compliance. HIPAA also authorizes state attorneys general to file suit on behalf of their residents. Courts may award damages, costs and attorneys’ fees related to violations of HIPAA in such cases. While HIPAA does not create a private right of action allowing individuals to sue us in civil court for violations of HIPAA, its standards have been used as the basis for duty of care in state civil suits such as those for negligence or recklessness in the misuse or breach of PHI.
HIPAA further has certain patient notification requirements for breaches or non-permitted use or disclosure of PHI, which include thresholds for reporting to HHS and local media, and such public reporting may also increase the risk of civil suits related to privacy incidents.
Numerous other federal and state laws and regulations protect the confidentiality, privacy, availability, integrity and security of PHI and other types of personal information. These laws and regulations are often uncertain, contradictory, and subject to changed or differing interpretations, and we expect new laws, rules and regulations regarding privacy, data protection, and information security to be proposed and enacted in the future, any of which could impact our business. For example, the California Consumer Privacy Act of 2018, as amended (the “CCPA”) affords consumers certain privacy protections and rights, including the right to request that a business delete their personal information unless it is necessary for the business to maintain for certain purposes, to direct a business to correct errors in their personal information, and to limit the use and disclosure of sensitive information. They have the right to know if their personal information is being sold or shared and the right to opt out of the “sale” or “sharing” of personal information, as those terms are defined under the CCPA. Further, the CCPA provides for civil penalties for violations, as well as a private right of action for data breaches that may increase data breach litigation. Compliance with the evolving landscape of privacy, data protection and information security laws and regulations could be time-consuming and expensive and require changes to our current processes and practices, and
any failure by us or our Medical Groups to comply with these and any other comprehensive privacy laws passed at the state or federal level may result in regulatory enforcement action, civil litigation and reputational harm.
While we have implemented data privacy and security measures in an effort to comply with applicable laws, regulations, and contractual obligations relating to privacy and data protection, some PHI and other personal information or confidential information is transmitted to us by third parties, who may not implement adequate security and privacy measures. Additionally, we transmit PHI and other personal information or confidential information to third parties, which carries the risk of breach despite our security and privacy measures. Further, any PHI or other personal information residing with a Privia Physicians’ Affiliated Practices or with our ACO participants may not be subject to adequate security and privacy measures, which may result in a breach of its Business Associate Agreement, or business associate agreement, with the relevant covered entity. Although a business associate may be independently found liable for a breach of the privacy or security requirements of HIPAA, we could also be held liable for such breach as the covered entity, result in government-imposed fines, orders requiring that we or these third parties change our or their practices, or criminal charges, any or all of which could adversely affect our business.
Additionally, we publish privacy policies and other documentation regarding our collection, processing, use and disclosure of personal information. Although we endeavor to comply with our published policies and other documentation, we may at times fail to do so or may be perceived to have failed to do so. Moreover, despite our efforts, we may not be successful in achieving compliance, including if our employees, contractors, service providers or vendors fail to comply with our published policies and documentation. Such failures can subject us to potential local, state and federal action if they are found to be deceptive, unfair, or misrepresentative of our actual practices. Claims that we have violated individuals’ privacy rights or failed to comply with data protection laws or applicable privacy notices, even if we are not found liable, could be expensive and time-consuming to defend, result in reputational harm, or have a material adverse impact on our business and our financial results.
Human Capital Risks
We depend on our senior management team and other key employees, and the loss of one or more of these employees or an inability to attract, recruit, motivate, develop and retain other highly skilled employees could harm our business.
Our success depends largely upon the continued services of our senior management team and other key employees. Employee attraction and retention may be difficult due to many factors, including fluctuations in economic and industry conditions; employee expectations; the effectiveness of our talent strategies and benefits and well-being programs, including compensation; the effectiveness of our training programs and our ability to effectively integrate employees into our business and operating model; and fluctuations in the labor market, including rising wages and competition for talent, which has increased due to persistent labor shortages and wage inflation. In addition, the shift to remote or hybrid work arrangements at many companies, including us, have significantly increased competition for highly-skilled personnel, who are no longer limited to opportunities within a particular geographic area. A lack of employee engagement, including as a result of working remotely, may reduce efficiency and productivity; increase turnover, burnout and absenteeism; and otherwise adversely affect our business and impede the achievement of our strategy. We rely on our leadership team in the areas of operations, provision of medical services, information technology and security, marketing, and general and administrative functions. From time to time, there may be changes to our management team resulting from the hiring or departure of executives or key employees, which could disrupt our business. Our employment agreements with our executive officers and other key personnel do not require them to continue to work for us for any specified period and, therefore, they could terminate their employment with us at any time. The loss of one or more of, or changes in, the members of our senior management team, or other key employees, could cause disruptions in, or harm to, our business. Furthermore, our business and results of operations could be adversely affected if we fail to adequately plan for and successfully carry out the succession of our key executives and senior leaders. For additional information, see “Business - Human Capital Resources.”
The operations and growth strategy of the Company and its Medical Groups depend on our ability to recruit and retain qualified talent, including physicians and non-physician practitioners.
The operations and growth strategy of the Company and its Medical Groups depend on our ability to recruit and retain qualified talent, including physicians and non-physician practitioners. Changes in the healthcare industry’s labor market have generally increased labor costs and competition for qualified and experienced individuals. In some markets in which our business operates or may consider operating, there are shortages of physicians, non-physician clinicians or other medical support personnel. We and our Medical Groups have experienced, and expect to continue to experience, difficulty in hiring and retaining qualified individuals at acceptable salary ranges. We may be required to enhance wages and benefits to recruit and retain physicians, non-physician clinicians and medical support personnel. If the Company and its Medical Groups are unable to recruit or retain a sufficient number of qualified personnel at an acceptable cost, we may not be able to fully implement our operating model in existing or new markets or execute our growth strategy.
In particular, the success of our business depends, in part, on the number, specialties, and quality of Privia Physicians, the utilization practices of these physicians, maintaining good relations with these physicians, and physician expenses, such as salary and medical malpractice expenses, as well as our ability to recruit a sufficient number of Privia Providers from the overall pool of physicians and non-physician practitioners and state-level restrictions on autonomous practice by non-physician practitioners. Our operating model and growth strategy rely on aggregating a sufficient number of Privia Physicians in each Medical Group, as the number of Privia
Physicians in a particular market impacts our attributed lives for VBC purposes, our costs and our Medical Groups’ costs, and our revenues from management services. The departure of a large number of Privia Physicians. certain of our Affiliated Practices or ACO participants could negatively impact our financial performance and ability to perform under our VBC arrangements. Further, the loss of any Privia Physician could result in that physician’s patient population shifting their care preferences to a non-Privia provider, which could negatively affect our revenues. We may not be able to recruit new providers to replace the services of the departing Privia Physician, and we may not be able to satisfy certain obligations under third-party payer programs. We and our Medical Groups face increased challenges recruiting and retaining quality physicians as the physician population reaches retirement age, particularly if there are shortages of physicians willing and able to provide comparable services. Further, the ability to recruit and contract with physicians is closely regulated. For example, the types, amount and duration of compensation and assistance that can be provided when recruiting physicians is limited by the federal Anti-Kickback Statute, the Stark Law, and other applicable laws and regulations intended to prevent fraud and abuse.
The Company and its Medical Groups continue to face increasing competition recruiting and retaining quality physicians and non-physician clinicians, including from health systems, independent physician practice management companies, and health insurers and private equity-backed companies seeking to acquire or affiliate with physicians or physician practices. Healthcare providers and companies with which we and our Medical Groups compete for personnel may have greater resources than we have. Our ability to recruit and retain physicians and non-physician clinicians may be negatively impacted if we are unable to provide adequate managerial support, support personnel, or technologically advanced equipment and facilities. In addition, continued uncertainty around the enforceability of non-compete restrictions under state and federal laws and regulations could impact our ability to recruit and retain physicians and non-physician practitioners. If we or our Medical Groups hire individuals formerly associated with competitors, their former employers may attempt to enforce non-compete provisions and similar restrictions, resulting in a diversion of our time and resources. Further, former employers may pursue legal claims against us or our Medical Groups on the basis of interference with contractual relationships. Any failure by us to hire and retain qualified personnel may negatively affect our results of operations, financial condition, and cash flows.
For additional risks related to attracting and retaining highly qualified personnel, see “We depend on our senior management team and other key employees, and the loss of one or more of these employees or an inability to attract, recruit, motivate, develop and retain other highly skilled employees could harm our business.”
Failure to attract and retain talent within our growth and business development teams could impede our growth.
We believe that our future growth will depend on the continued development of our growth team and its ability to obtain new Privia Physicians while our implementation team and practice consultants manage existing affiliate physician relationships. Additionally, we rely upon our business development staff to identify and develop potential relationships with new Medical Groups and health system or hospital partners. Identifying and recruiting qualified personnel and training them requires significant time, expense and attention especially given the complexity of our business and the Privia operating model. It can take six months or longer before a new sales representative is fully trained and productive. Our business may be adversely affected if our efforts to expand and train our direct sales force and business development staff do not generate a corresponding increase in revenue. In particular, if we are unable to hire and develop sufficient numbers of productive direct sales and business development personnel or if new personnel are unable to achieve desired productivity levels in a reasonable period of time, our expected growth will be impeded.
Our corporate culture has contributed to our success, and if we cannot maintain this culture as we grow, we could lose the innovation, creativity and teamwork fostered by our culture and our business may be harmed.
We believe that our culture has been and will continue to be a critical contributor to our success. We expect to continue to hire aggressively as we expand, and we believe our corporate culture has been crucial in our success and our ability to attract highly skilled personnel. If we do not continue to develop our corporate culture or maintain and preserve our core values as we grow and evolve, we may be unable to foster the innovation, curiosity, creativity, focus on execution, teamwork and the facilitation of critical knowledge transfer and knowledge sharing we believe we need to support our growth. Moreover, liquidity available to our employee security holders could lead to disparities of wealth among our employees, which could adversely impact relations among employees and our culture in general.
For additional risks related to our corporate culture, see “We depend on our senior management team and other key employees, and the loss of one or more of these employees or an inability to attract, recruit, motivate, develop and retain other highly skilled employees could harm our business.”
Financial Risks
We have a history of net losses, we anticipate increasing expenses in the future, and we may not be able to maintain profitability.
We have incurred losses in the past and continue to have an accumulated deficit. To date, we have financed our operations principally from revenue earned from our Medical Groups’ billing and collection for healthcare services furnished by Privia Providers, revenues earned from VBC arrangements with our ACOs, the incurrence of indebtedness and the sale of our equity. We may not generate positive cash flow from operations or achieve profitability in any given period, and our limited operating history may make it difficult for you to evaluate our current business and our future prospects.
We have encountered and will continue to encounter risks and difficulties frequently experienced by growing companies in rapidly changing industries, including increasing expenses as we continue to grow our business. We expect our operating expenses to increase as we continue to hire additional personnel, expand our operations and infrastructure, and continue to expand to reach more patients. These investments may be more costly than we expect, and if we do not achieve the benefits anticipated from these investments, or if the realization of these benefits is delayed, they may not result in increased revenue or growth in our business. If our growth rate were to decline significantly or become negative, it could adversely affect our financial condition and results of operations. If we are not able to maintain positive cash flow in the long term, we may require additional financing, which may not be available on favorable terms or at all, which could be dilutive to our stockholders. If we are unable to successfully address these risks and challenges as we encounter them, our business, results of operations and financial condition could be adversely affected. Our failure to achieve or maintain profitability could negatively impact the value of our common stock.
Our ability to use our net operating losses to offset future taxable income may be subject to certain limitations.
In general, under Section 382 of the Internal Revenue Code of 1986, as amended (the “Code”), a corporation that undergoes an “ownership change” is subject to limitations on its ability to utilize its pre-change NOLs to offset future taxable income or taxes. A Code Section 382 ownership change generally occurs if one or more stockholders or groups of stockholders who own at least 5% of a corporation’s stock increase their ownership by more than 50 percentage points over their lowest ownership percentage within a rolling three-year period. Similar rules may apply under state tax laws. As of December 31, 2025, we had approximately $26.9 million of federal and $24.7 million of state (post-apportioned state NOL) NOL carryforwards. During the year ended December 31, 2025, we utilized the remaining federal NOL carryforwards for years before 2018 which would have otherwise began to expire in 2034. All remaining federal NOL carryforwards are indefinite-lived. The state NOL carryforwards begin to expire in 2034. Changes in the ownership of our stock in the future, including as a result of future offerings, and some of which are outside of our control, could result in an ownership change under Section 382 of the Code (or applicable state law) after such date, which could significantly limit our ability to utilize our existing and future NOL carryforwards arising at any time prior to such ownership change.
We face risks associated with our indebtedness, which could restrict our current and future operations or adversely affect our business and growth prospects.
As of December 31, 2025, there was no amount outstanding under our Revolving Credit Facility, which has $125.0 million of borrowing availability. Any indebtedness we may incur could require us to divert funds identified for other purposes for debt service and impair our liquidity position. If we cannot generate sufficient cash flow from operations to service any indebtedness we may incur, we may need to restructure or refinance our debt, reduce or delay capital expenditures, dispose of assets or issue equity to obtain necessary funds. We cannot assure you that we will be able to refinance any of our indebtedness on a timely basis, on satisfactory or commercially reasonable terms or at all. There can be no assurance that we will be able to obtain sufficient funds to enable us to repay or refinance our debt obligations on commercially reasonable terms, or at all. Additionally, our Revolving Credit Agreement contains a number of restrictive covenants that impose significant operating and financial restrictions on us and may limit our ability to engage in acts that may be in our long-term best interests, including restrictions on our ability to:
•incur additional indebtedness or other contingent obligations;
•create liens;
•make investments, acquisitions, loans and advances;
•consolidate, merge, liquidate or dissolve;
•sell, transfer or otherwise dispose of our assets;
•pay dividends on our equity interests or make other payments in respect of capital stock; and
•materially alter the business we conduct.
The restrictive covenants in the Revolving Credit Agreement require us to satisfy certain financial condition tests, as described in “Management’s Discussion and Analysis of Financial Condition and Results of Operations” of this Annual Report on Form 10-K. Our ability to satisfy those tests can be affected by events beyond our control.
A breach of the covenants or restrictions under the Revolving Credit Agreement could result in an event of default, which could allow the creditors to accelerate the related debt. Any failure to make payments of interest and principal on any future outstanding indebtedness on a timely basis would likely result in penalties or defaults, which would also harm our ability to incur additional indebtedness. Fluctuations in interest rates could also increase borrowing costs, impact the amount of interest we could be required to pay and reduce earnings accordingly. In addition, developments in tax policy, such as the disallowance of tax deductions for interest paid on outstanding indebtedness, could have an adverse effect on our liquidity and our business, financial condition and results of operations.
Our failure to raise additional capital or generate cash flows necessary to expand our operations and invest in new technologies in the future could reduce our ability to compete successfully and harm our results of operations.
We may need to raise additional funds, and we may not be able to obtain additional debt or equity financing on favorable terms or at all. If we raise additional equity financing, our security holders may experience significant dilution of their ownership interests. If we engage in additional debt financing, we may be required to accept terms that restrict our ability to incur additional indebtedness, force us to maintain specified liquidity or other ratios or restrict our ability to pay dividends or make acquisitions. In addition, the covenants in our Revolving Credit Agreement may limit our ability to obtain additional debt, and any failure to adhere to these covenants could result in penalties or defaults that could further restrict our liquidity or limit our ability to obtain financing. Any failure to obtain additional capital on acceptable terms, or at all, could limit our operational flexibility, including our ability to:
•develop and enhance our patient services;
•continue to expand our organization;
•hire, train and retain employees;
•respond to competitive pressures or unanticipated working capital requirements; or
•pursue acquisition opportunities.
As a public company, we are obligated to maintain proper and effective internal control over financial reporting in order to comply with Section 404 of the Sarbanes-Oxley Act. If we fail to maintain effective internal control over financial reporting, we may not be able to report our financial results in a timely or accurate manner, which may adversely affect investor confidence in us.
As a public company, we are required to document and test our internal control over financial reporting pursuant to Section 404 of the Sarbanes-Oxley Act so that our management can certify as to the effectiveness of our internal control over financial reporting. Section 404(a) of the Sarbanes-Oxley Act (“Section 404(a)”) requires that management assess and report annually on the effectiveness of our internal control over financial reporting and identify any material weaknesses in our internal control over financial reporting. Section 404(b) of the Sarbanes-Oxley Act requires our independent registered public accounting firm to issue an annual report that addresses the effectiveness of our internal control over financial reporting. Our compliance with Section 404(a) has required us to incur substantial expenses and expend significant management efforts.
If we identify material weaknesses in our internal control over financial reporting in the future, our management will be unable to assert that our disclosure controls and procedures and our internal control over financial reporting is effective. If we are unable to assert that our internal control over financial reporting is effective, or if our independent registered public accounting firm is unable to express an unqualified opinion as to the effectiveness of our internal control over financial reporting, investors may lose confidence in the accuracy and completeness of our financial reports, the market price of our common stock could be adversely affected and we could become subject to litigation or investigations by Nasdaq, the SEC, or other regulatory authorities, which could require additional financial and management resources.
General Risks
A deterioration of public health conditions associated with a pandemic, epidemic or outbreak of an infectious disease in the markets in which we operate could adversely impact our business.
If a pandemic, epidemic, outbreak of infectious disease, or other widespread health crisis, such as the COVID-19 pandemic, affects our markets, our business and operations could be adversely affected. Any such event could diminish public confidence in healthcare facilities and providers, particularly those involved in treating affected patients, potentially changing the utilization of healthcare services. If any of our Medical Groups, Privia Providers or ACO participants are involved, or perceived as being involved, in treating patients with an infectious disease, patients might avoid seeking care or cancel elective procedures. Economic instability caused by such a health crisis, has and could lead to a decline in overall patient volumes or an increase in the number of uninsured and underinsured. In addition, a pandemic, epidemic or outbreak might adversely affect the business and operations of the Company, its Medical Groups or ACO participants by causing a temporary shutdown or diversion of patients from our Medical Groups or ACO participants, causing disruptions or delays in supply chains for materials and products, or by causing staffing shortages, like those experienced during the COVID-19 pandemic. Such disruptions could hinder our ability to implement clinical initiatives to manage healthcare conditions of patients and appropriately document patient risk profiles, adversely impacting our ability to accurately project medical cost trends, increase patients’ clinical disease burdens or reduce preventive care. Although we have business resiliency plans to address circumstances including a future pandemic, the potential impact of, as well as the response of the public and applicable governments to, a future pandemic, epidemic or outbreak is difficult to predict and could adversely affect our business, results of operations, and financial condition.
Increased attention to, and evolving expectations for, environmental, social, and governance (“ESG”) initiatives could increase our costs, harm our reputation, or otherwise adversely impact our business.
Companies across industries are facing increasing scrutiny from a variety of stakeholders related to their ESG and sustainability practices. ESG initiatives and disclosures may result in increased costs (including but not limited to increased costs related to
compliance, stakeholder engagement, contracting and insurance), enhanced compliance or disclosure obligations, or other adverse impacts to our business, financial condition, or results of operations.
While we may at times engage in certain ESG initiatives (such as voluntary or required disclosures or certifications), such initiatives may be costly and may not have the desired effect. Moreover, we may not be able to successfully complete such initiatives due to factors that are within or outside of our control. Even if this is not the case, our actions may subsequently be determined to be insufficient by various stakeholders, and we may be subject to investor or regulator scrutiny on our ESG efforts. To the extent ESG matters negatively impact our reputation, it may also impede our ability to compete as effectively to attract and retain employees, which may adversely impact our operations. In addition, we continue to evaluate our ESG disclosure practices in light of increasing levels of regulation with respect to ESG matters, such as the California Corporate Climate Data Accountability Act and Climate-Related Financial Risk and similar bills under consideration in other U.S. states, which may require us to incur significant additional costs to comply, and impose increased oversight obligations on our management and board of directors.
Risks Related to Our Common Stock
Provisions of our corporate governance documents could make an acquisition of us more difficult and may prevent attempts by our stockholders to replace or remove our current management, even if beneficial to our stockholders.
Our amended and restated certificate of incorporation and amended and restated bylaws and the Delaware General Corporation Law (the “DGCL”) contain provisions that could make it more difficult for a third-party to acquire us, even if doing so might be beneficial to our stockholders. Among other things, these provisions:
•allow us to authorize the issuance of undesignated preferred stock, the terms of which may be established and the shares of which may be issued without stockholder approval, and which may include supermajority voting, special approval, dividend, or other rights or preferences superior to the rights of stockholders;
•provide for a classified board of directors with staggered three-year terms;
•prohibit stockholder action by written consent and stockholder special meetings as well as permit removal of directors only for cause; and
•establish advance notice requirements for nominations for elections to our Board or for proposing matters that can be acted upon by stockholders at stockholder meetings.
Our amended and restated certificate of incorporation contains a provision that provides us with protections similar to Section 203 of the DGCL, and will prevent us from engaging in a business combination with a person unless board or stockholder approval is obtained prior to the acquisition. These provisions could discourage, delay or prevent a transaction involving a change in control of our company. These provisions could also discourage proxy contests and make it more difficult for you and other stockholders to elect directors of your choosing and cause us to take other corporate actions you desire, including actions that you may deem advantageous, or negatively affect the trading price of our common stock. In addition, because our Board is responsible for appointing the members of our management team, these provisions could in turn affect any attempt by our stockholders to replace current members of our management team.
These and other provisions in our amended and restated certificate of incorporation, amended and restated bylaws and Delaware law could make it more difficult for stockholders or potential acquirers to obtain control of our Board or initiate actions that are opposed by our then-current Board, including delay or impede a merger, tender offer or proxy contest involving our company. The existence of these provisions could negatively affect the price of our common stock and limit opportunities for you to realize value in a corporate transaction.
Our amended and restated certificate of incorporation designates the Court of Chancery of the State of Delaware as the exclusive forum for certain litigation that may be initiated by our stockholders, which may limit our stockholders’ ability to obtain a favorable judicial forum for disputes with us.
Pursuant to our amended and restated certificate of incorporation, unless we consent in writing to the selection of an alternative forum, the Court of Chancery of the State of Delaware is the sole and exclusive forum for (1) any derivative action or proceeding brought on our behalf, (2) any action asserting a claim of breach of a fiduciary duty owed by any of our directors, officers or other employees to us or our stockholders, (3) any action asserting a claim against us arising pursuant to any provision of the DGCL, our amended and restated certificate of incorporation or our amended and restated bylaws or (4) any other action asserting a claim against us that is governed by the internal affairs doctrine; provided that for the avoidance of doubt, the forum selection provision that identifies the Court of Chancery of the State of Delaware as the exclusive forum for certain litigation, including any “derivative action”, will not apply to suits to enforce a duty or liability created by the Securities Act, the Exchange Act or any other claim for which the federal courts have exclusive jurisdiction. Our amended and restated certificate of incorporation further provides that any person or entity purchasing or otherwise acquiring any interest in shares of our capital stock is deemed to have notice of and consented to the provisions of our amended and restated certificate of incorporation described above. The forum selection clause in our amended and restated certificate of incorporation may have the effect of discouraging lawsuits against us or our directors and officers and may limit our stockholders’ ability to obtain a favorable judicial forum for disputes with us.
Our operating results and stock price may be volatile, and the market price of our common stock may drop below the price you pay.
Our quarterly operating results are likely to fluctuate in the future. In addition, securities markets worldwide have experienced, and are likely to continue to experience, significant price and volume fluctuations. This market volatility, as well as general economic, market or political conditions, could subject the market price of our shares to wide price fluctuations regardless of our operating performance. Our operating results and the trading price of our shares may fluctuate in response to various factors, including:
•market conditions in our industry or the broader stock market;
•actual or anticipated fluctuations in our quarterly financial and operating results;
•introduction of new solutions or services by us or our competitors;
•the operating and stock price performance of comparable companies;
•issuance of new or changed securities analysts’ reports or recommendations;
•sales, or anticipated sales, of large blocks of our stock;
•additions or departures of key personnel;
•regulatory or political developments;
•litigation and governmental investigations;
•changing economic conditions;
•negative publicity relating to us or our competitors;
•investors’ perception of us;
•events beyond our control such as extreme weather and geopolitical conflicts; and
•any default on our indebtedness.
These and other factors, many of which are beyond our control, may cause our operating results and the market price and demand for our shares to fluctuate substantially. Fluctuations in our quarterly operating results could limit or prevent investors from readily selling their shares and may otherwise negatively affect the market price and liquidity of our shares. In addition, the trading market for our shares may be subject to increased volatility. In addition, in the past, when the market price of a stock has been volatile, holders of that stock have sometimes instituted securities class action litigation against the company that issued the stock. If any of our stockholders brought a lawsuit against us, we could incur substantial costs defending the lawsuit. Such a lawsuit could also divert the time and attention of our management from our business, which could significantly harm our profitability and reputation.
Future sales and issuances of our outstanding shares could cause the market price of our common stock to drop significantly, even if our business is doing well.
Sales of a substantial number of shares of our common stock in the public market have occurred and could occur at any time. These sales, or the perception in the market that the holders of a large number of shares intend to sell shares, could reduce the market price of our common stock. All of our common stock sold pursuant to an offering covered by a registration statement, including common stock sold by stockholders rather than the Company, will be freely transferable. In addition, shares of our common stock issued or issuable under our equity incentive plans to employees and directors have been registered on one or more Form S-8 registration statements and may be freely sold in the public market upon issuance, except for shares held by affiliates who have certain restrictions on their ability to sell. The market price of our stock could decline if the holders of our shares of common stock sell them or are perceived by the market as intending to sell them.
Because we have no current plans to pay regular cash dividends on our common stock, you may not receive any return on investment unless you sell your common stock for a price greater than that which you paid for it.
We do not anticipate paying any regular cash dividends on our common stock. Any decision to declare and pay dividends in the future will be made at the discretion of our Board and will depend on, among other things, our results of operations, financial condition, cash requirements, contractual restrictions and other factors that our Board may deem relevant. In addition, our ability to pay dividends is, and may be, limited by covenants of existing and any future outstanding indebtedness we or our subsidiaries incur. Therefore, any return on investment in our common stock is solely dependent upon the appreciation of the price of our common stock on the open market, which may not occur. For additional information, see “Market for Registrant’s Common Equity, Related Stockholder Matters and Issuer Purchases of Equity Securities - Dividend Policy.”
ITEM 1B. UNRESOLVED STAFF COMMENTS
None.
ITEM 1C. CYBERSECURITY
Item 106(b) Cybersecurity Risk Management and Strategy
Information and Cybersecurity Risk Management and Strategy
Our approach to risk management, including cybersecurity risk, is designed to identify, assess, prioritize and manage major risk exposures that could affect our ability to execute our corporate strategy and fulfill our business objectives. Our cybersecurity risk management program is designed based on industry standards and informed by the National Institute of Standards and Technology Cybersecurity Framework. We perform risk assessments in which we map and prioritize identified cybersecurity risks, including risks associated with our use of third- and fourth-party vendors, Medical Groups, Privia Providers and their Affiliated Practices, based on probability, immediacy and potential magnitude. These assessments inform our cybersecurity risk management strategies and oversight processes, and we view cybersecurity risks as one of the key risk categories we face.
Our processes for assessing, identifying and managing cybersecurity risks and vulnerabilities are embedded across our business as part of our enterprise risk management (“ERM”) program. Among other things, we regularly engage with internal and external cybersecurity assessors, consultants and auditors to enhance our cybersecurity risk management strategies, review compliance with evolving standards and evaluate the effectiveness and maturity of our controls and perform regular internal and external risk assessments including those required by HIPAA; provide annual mandatory privacy and security training for all employees; perform technical testing and penetration testing to validate the effectiveness of our cybersecurity program; and perform simulated breach testing and tabletop exercises to simulate responses to information security incidents. We have established processes to oversee and manage risks associated with our third- and certain fourth-party vendors, including regular security assessments and compliance reviews. We use the findings from these and other processes to assess our information and cybersecurity practices, procedures and technologies, including for potential enhancements to our risk mitigation strategies. Our Cybersecurity Incident Response Plan (“CSIRP”), which includes processes to detect triage, assess the severity of, escalate, contain, investigate and resolve or mitigate cybersecurity incidents, as well as to comply with applicable legal obligations and mitigate brand and reputational damage. In addition, we maintain cyber liability insurance to protect against potential losses arising from cybersecurity incidents. In 2025, we did not identify any cybersecurity threats or incidents, including as a result of any prior cybersecurity incidents, that have materially affected or are reasonably likely to materially affect us, including our operations, business strategy, results of operations, or financial condition. However, despite our efforts, we cannot eliminate all risks from cybersecurity threats or incidents or provide assurances that we have not experienced an undetected cybersecurity threat or incident. For more information about these risks, please see “Item 1A - Risk Factors” under the caption “Security threats, cybersecurity incidents or other forms of data breaches, catastrophic events and other disruptions to our, our Medical Groups’, our business partners’ or our vendors’ information technology and related systems could compromise sensitive information related to our business, the Medical Groups or patients, prevent access to critical information, harm patients, require remediation and other corrective action, which can be expensive, and expose us to liability, which could adversely affect our business, operations and reputation. ” of this Annual Report on Form 10-K.
Information and Cybersecurity Governance and Oversight
Our Board of Directors (“Board”) is responsible for overseeing risk management at Privia and, as part of this responsibility, the Board, assisted by its committees, exercises oversight over our ERM program which is designed and implemented by management. As part of its broader risk oversight activities, the Board oversees risks from cybersecurity threats, both directly and through the Audit Committee of the Board (“Audit Committee”) and Compliance Committee of the Board (“Compliance Committee”). The Compliance Committee is responsible for reviewing data security programs, including cybersecurity and procedures regarding disaster recovery and critical business continuity. The Compliance Committee is also responsible for reviewing Privia’s programs and plans established by management to monitor compliance with data security compliance programs and test preparedness. The Audit Committee assists our Board in fulfilling its oversight responsibilities with respect to risk management in the areas of internal control over financial reporting, disclosure controls and procedures, and legal and regulatory compliance, and discusses with management policies and practices with respect to risk assessment and risk management.
The Compliance Committee receives quarterly reports from the Chief Information Security Officer (“CISO”) and Privacy Officer on information security risks, including cybersecurity incidents or privacy events, relevant information about the cybersecurity threat landscape, and updates on our cybersecurity risk management strategy and any potential issues. The Compliance Committee reports to the Audit Committee at each regularly scheduled meeting of the Audit Committee, and the Compliance and Audit Committee meet periodically in joint session to discuss matters of joint interest and responsibility, such as cybersecurity risks. In addition, the full Board receives periodic briefings on cybersecurity risks from the CISO.
Our CISO, who leads our information security team and reports to our Chief Technology Officer, is responsible for day-to-day identification, assessment and management of the information security risks we face. The CISO provides monthly information and cybersecurity updates to a cross-functional team of executive leaders, who prioritize risks and risk mitigation activities. The CISO has
held executive technology leadership roles within health systems and physician groups for over 15 years, including Chief Technology Officer, Chief Information Officer, and Chief Information Security Officer. The information security team works with our broader technology team, as well as our compliance and legal teams, to align operations and technology developments with cybersecurity program objectives.
In addition, we maintain processes for managing incident assessment and internal escalation. We have established a Cybersecurity Incident Response Team (“CSIRT”), which is responsible for (1) responding to cybersecurity incidents, (2) maintaining our CSIRP that is regularly updated in response to organizational changes, technical changes, changes to the threat landscape or in response to active or previous cybersecurity incidents, and (3) monitoring the prevention, detection, mitigation, and remediation of cybersecurity incidents. The CSIRT is comprised of the CISO and other key members of management, including the Privacy Officer, Chief Technology Officer, Chief Audit and Compliance Officer, General Counsel and other members of management and our technical response teams as necessary to appropriately respond to an incident, including mitigation, remediation and any required or recommended disclosure of an incident. Furthermore, as part of management’s oversight of information and cybersecurity risks, we maintain a Third Party Access Committee, comprised of our CISO, Privacy Officer, Chief Technology Officer and colleagues drawn from across the organization, including our technology, compliance and legal teams, which is responsible for reviewing and monitoring compliance for third- and certain fourth-party requests for and access to certain Company data and information.
ITEM 2. PROPERTIES
Our headquarters is located in Arlington, Virginia. Our lease on this space expires on December 31, 2031. We have also leased space for our other offices throughout the United States. We believe that our headquarters and other offices are adequate for our immediate needs and that additional or substitute space is available if needed to accommodate growth and expansion.
ITEM 3. LEGAL PROCEEDINGS
We are currently involved in, and may in the future become involved in, legal proceedings, claims and investigations in the ordinary course of our business, including medical malpractice claims. These claims or proceedings can involve various types of parties, including governments, competitors, customers, partners, suppliers, service providers, licensees, licensors, employees, or stockholders, among others. Although the results of these legal proceedings, claims and investigations cannot be predicted with certainty, we do not believe that the final outcome of any matters that we are currently involved in are reasonably likely to have a material adverse effect on our business, financial condition or results of operations. Regardless of final outcomes, however, any such proceedings, claims, and investigations may nonetheless impose a significant burden on management and employees and be costly to defend, with unfavorable preliminary or interim rulings.
ITEM 4. MINE SAFETY DISCLOSURES
Not applicable.
PART II
ITEM 5. MARKET FOR REGISTRANT'S COMMON EQUITY, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES
Market Information
Our common stock has been listed on the Nasdaq Global Select Market under the symbol “PRVA” since April 29, 2021. Prior to that, there was no public trading market for our common stock.
Holders of Record
As of the close of business on February 20, 2026, there were approximately 16 stockholders of record of our common stock. The actual number of stockholders is greater than this number of record holders, and includes stockholders who are beneficial owners, but whose shares are held in street name by brokers and other nominees. This number of holders of record also does not include stockholders whose shares may be held in trust by other entities.
Stock Performance Graph -
The following performance graph and related information shall not be deemed to be “filed” for purposes of Section 18 of the Exchange Act, or otherwise subject to the liabilities of that section or Sections 11 and 12(a)(2) of the Securities Act of 1933, as amended, and shall not be incorporated by reference into any registration statement or other document filed by us with the SEC, whether made before or after the date of this Annual Report on Form 10-K, regardless of any general incorporation language in such filing, except as shall be expressly set forth by specific reference in such filing.
The following graph and related information show a comparison of the cumulative total return for our common stock, Russell 2000 Index, and NASDAQ Health Care Index between April 28, 2021 (the date our common stock commenced trading on the NASDAQ) through December 31, 2025. All values assume an initial investment of $100 and reinvestment of any dividends. The comparisons are based on historical data and are not indicative of, nor intended to forecast, the future performance of our common stock.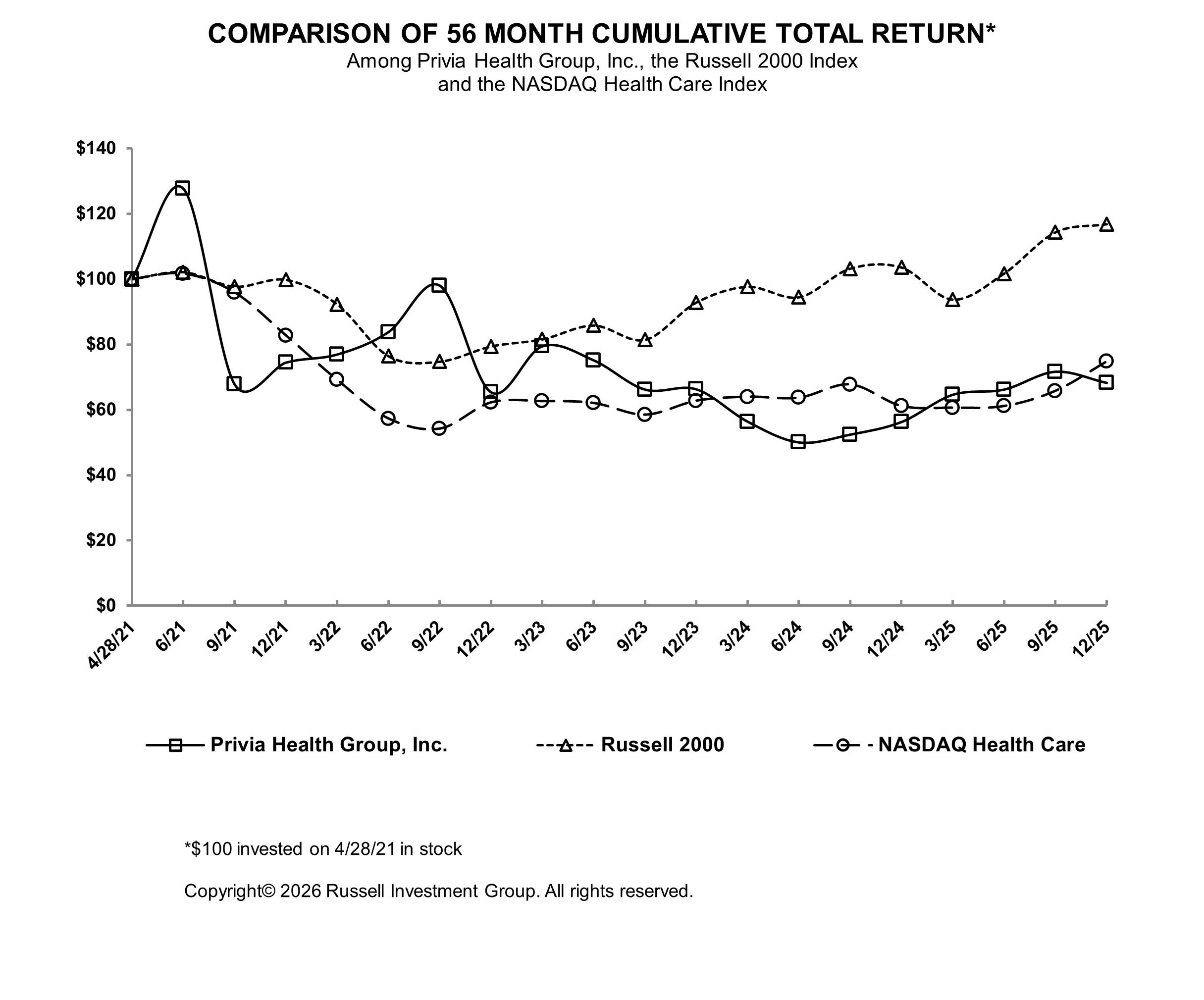
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | 4/28/2021 | | 6/30/2021 | | 9/30/2021 | | 12/31/2021 | | | | | | | | | | | | | | | | |
Privia Health Group, Inc. (1) | | $ | 100.00 | | | $ | 127.68 | | | $ | 67.80 | | | $ | 74.45 | | | | | | | | | | | | | | | | | |
| Russell 2000 | | $ | 100.00 | | | $ | 102.15 | | | $ | 97.69 | | | $ | 99.79 | | | | | | | | | | | | | | | | | |
| NASDAQ Health Care | | $ | 100.00 | | | $ | 101.67 | | | $ | 95.90 | | | $ | 82.74 | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | |
| | 3/31/2022 | | 6/30/2022 | | 9/30/2022 | | 12/31/2022 | | | | | | | | | | | | | | | | |
Privia Health Group, Inc. (1) | | $ | 76.92 | | | $ | 83.80 | | | $ | 98.01 | | | $ | 65.35 | | | | | | | | | | | | | | | | | |
| Russell 2000 | | $ | 92.28 | | | $ | 76.41 | | | $ | 74.74 | | | $ | 79.39 | | | | | | | | | | | | | | | | | |
| NASDAQ Health Care | | $ | 69.12 | | | $ | 57.28 | | | $ | 54.19 | | | $ | 62.22 | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | |
| | 3/31/2023 | | 6/30/2023 | | 9/30/2023 | | 12/31/2023 | | | | | | | | | | | | | | | | |
Privia Health Group, Inc. (1) | | $ | 79.45 | | | $ | 75.14 | | | $ | 66.19 | | | $ | 66.27 | | | | | | | | | | | | | | | | | |
| Russell 2000 | | $ | 81.57 | | | $ | 85.81 | | | $ | 81.41 | | | $ | 92.83 | | | | | | | | | | | | | | | | | |
| NASDAQ Health Care | | $ | 62.61 | | | $ | 62.04 | | | $ | 58.45 | | | $ | 62.73 | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | |
| | 3/31/2024 | | 6/30/2024 | | 9/30/2024 | | 12/31/2024 | | | | | | | | | | | | | | | | |
Privia Health Group, Inc. (1) | | $ | 56.37 | | | $ | 50.01 | | | $ | 52.40 | | | $ | 56.26 | | | | | | | | | | | | | | | | | |
| Russell 2000 | | $ | 97.64 | | | $ | 94.44 | | | $ | 103.20 | | | $ | 103.54 | | | | | | | | | | | | | | | | | |
| NASDAQ Health Care | | $ | 63.95 | | | $ | 63.66 | | | $ | 67.72 | | | $ | 61.13 | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | |
| | 3/31/2025 | | 6/30/2025 | | 9/30/2025 | | 12/31/2025 | | | | | | | | | | | | | | | | |
Privia Health Group, Inc. (1) | | $ | 64.60 | | | $ | 66.19 | | | $ | 71.65 | | | $ | 68.23 | | | | | | | | | | | | | | | | | |
| Russell 2000 | | $ | 93.73 | | | $ | 101.70 | | | $ | 114.30 | | | $ | 116.81 | | | | | | | | | | | | | | | | | |
| NASDAQ Health Care | | $ | 60.61 | | | $ | 61.10 | | | $ | 65.75 | | | $ | 74.75 | | | | | | | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | |
(1) $100 invested on April 28, 2021 in shares and in indices | | | | | | |
The information above shall not be deemed “soliciting material” or to be “filed” for purposes of Section 18 of the Exchange Act, or otherwise subject to the liabilities under that section, and shall not be incorporated by reference into any of our other filings under the Exchange Act, or the Securities Act of 1933, as amended, regardless of any general incorporation language in those filings.
Securities Authorized for Issuance under Equity Compensation Plans
The information required by this item will be set forth in the Proxy Statement and is incorporated into this Annual Report on Form 10-K by reference.
Recent Sales of Unregistered Securities
There were no unregistered sales of equity securities during the year ended December 31, 2025.
Dividend Policy
We currently intend to retain all available funds and any future earnings to fund the development and growth of our business and to repay indebtedness; therefore, we do not anticipate paying any cash dividends in the foreseeable future. Additionally, because we are a holding company, our ability to pay dividends on our common stock may be limited by restrictions on the ability of our subsidiaries to pay dividends or make distributions to us. Any future determination to pay dividends will be at the discretion of our Board, subject to compliance with covenants in current and future agreements governing our and our subsidiaries’ indebtedness, and will depend on our results of operations, financial condition, capital requirements and other factors that our Board may deem relevant.
Issuer Purchases of Equity Securities
None.
ITEM 6. [RESERVED]
ITEM 7. MANAGEMENT’S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS
The following discussion should be read in conjunction with our consolidated financial statements and accompanying notes included elsewhere in this Annual Report on Form 10-K. In addition, the following discussion and analysis and information contains forward-looking statements about the business, operations and financial performance of the Company based on our current expectations that involve risks, uncertainties and assumptions. Our actual results could differ materially from those anticipated by these forward-looking statements as a result of many factors. including, but not limited to, those identified below and those discussed in the sections titled “Risk Factors” and “Information Regarding Forward-Looking Statements” in this Annual Report on Form 10-K.
Overview
Privia Health is a technology-driven, national physician-enablement company that collaborates with physician practices, health plans, and health systems to achieve the quadruple aim of better outcomes, lower costs, improved patient experience, and happier and more engaged providers. We seek to accomplish the quadruple aim by entering markets and organizing existing physicians and non-physician clinicians into a unique practice model that combines the advantages of a partnership in a large regional Medical Group with significant provider autonomy for Privia Providers joining our Medical Groups.
Under our Privia Medical Group model, Privia Physicians join the Medical Group in their geographic market as an owner of the Medical Group. We own a majority interest in certain of our Medical Groups, with Privia Physicians collectively owning a minority interest, and we own no interest in certain other Non-Owned Medical Groups. In those markets in which state regulations do not allow us to own Medical Groups, the Non-Owned Medical Groups may be owned by the Privia Physicians or owned indirectly by a licensed physician holding a Privia leadership position, otherwise referred to as a Friendly Medical Group. Privia Physicians furnish healthcare services through our Medical Groups and continue to own their Affiliated Practices, which provide certain services to the Medical Groups, such as use of space, non-physician staffing, equipment and supplies.
We provide management services to the Medical Groups through a local MSO, which provides Medical Groups with access to VBC opportunities either directly or through Privia-owned ACOs. We have national committees that distribute quality guidance, and we employ Chief Medical Officers who provide clinical oversight and direction over the clinical affairs of the Owned Medical Groups. Additionally, we hold the provider contracts, maintain the patient records, set reimbursement rates, and negotiate payer contracts on behalf of the Owned Medical Groups.
In some instances, we also move into and expand in new and existing markets through our Privia Care Partners model, which offers an affiliation model to providers who are looking solely for VBC solutions. For those practices, we furnish population health services, reporting and analytics, along with certain management.
GAAP Financial Measures
• Revenue was $2.12 billion, $1.74 billion and $1.66 billion for the years ended December 31, 2025, 2024, and 2023, respectively.
• Operating income was $34.2 million, $17.0 million and $20.6 million for the years ended December 31, 2025, 2024, and 2023, respectively; and
• Net income attributable to Privia Health Group, Inc. was $22.9 million, $14.4 million and $23.1 million for the years ended December 31, 2025, 2024, and 2023, respectively.
Key Metrics and Non-GAAP Financial Measures
• Practice Collections were $3.47 billion, $2.97 billion and $2.84 billion for the years ended December 31, 2025, 2024, and 2023, respectively;
• Care Margin was $462.2 million, $403.9 million and $359.2 million for the years ended December 31, 2025, 2024, and 2023, respectively;
• Platform Contribution was $234.8 million, $195.6 million and $173.5 million for the years ended December 31, 2025, 2024, and 2023, respectively;
• Adjusted EBITDA was $125.5 million, $90.5 million and $72.2 million for the years ended December 31, 2025, 2024, and 2023, respectively.
See “Key Metrics” and “Non-GAAP Financial Measures” for more information as to how we define and calculate Implemented Providers, Attributed Lives, Practice Collections, Care Margin, Platform Contribution, Platform Contribution Margin, Adjusted EBITDA and Adjusted EBITDA Margin, and for a reconciliation of Gross Profit, the most comparable GAAP measure, to Care Margin, Gross Profit, the most comparable GAAP measure, to Platform Contribution, and net income, the most comparable GAAP measure, to Adjusted EBITDA.
Our Revenue
We recognize revenue from multiple stakeholders, including health care consumers, health insurers, employers, providers and health systems. Our revenue includes (i) FFS revenue generated from providing healthcare services to patients through Privia Providers of Owned Medical Groups or administrative fees collected for providing administrative services to Non-Owned Medical Groups, (ii) VBC revenue collected on behalf of our providers, primarily capitated revenue, shared savings (including surplus payments, shared savings, total cost of care budget payments and similar payments) and PMPM fees (including care management fees, management services fees, care coordination fees and all other similar administrative fees), and (iii) other revenue from additional services, such as concierge services, virtual visits, virtual scribes and coding.
FFS Revenue
We generate FFS-patient care revenue when we collect reimbursements for FFS medical services provided by Privia Providers. Our multi-year agreements with our providers have historically experienced a 96% provider retention rate, which leads to a highly predictable and recurring revenue model. Our FFS contracts with payer partners typically contain annual rate inflators and given our scale, enhanced commercial FFS rates in each of our markets. As a result of receiving these rate inflators and enhancements and if we continue to be successful in expanding our provider base, we expect revenue will grow year-over-year in absolute dollars. In addition, in our FFS-patient care revenue, we generate revenue from ancillary services such as clinical laboratory, imaging and pharmacy operations. Lastly, we also generate FFS-administrative services revenue by providing administration and management services to medical groups which are not owned or consolidated by us. FFS-patient care revenue represented 64.1%, 66.0% and 58.9% of total revenue for the years ended December 31, 2025, 2024, and 2023, respectively. FFS-administrative services revenue represented 6.5%, 7.2% and 6.8% of total revenue for the years ended December 31, 2025, 2024, and 2023, respectively.
VBC Revenue
Over time, we create incremental value for our provider partners by enabling them to succeed in VBC arrangements. We generate VBC revenue when our providers are reimbursed through traditional FFS Medicare, MSSP, Medicare Advantage, commercial payers and other existing and emerging direct payer and employer contracting programs. We monitor capitated and downside risk contracts and renegotiate or restructure as necessary as new information emerges. VBC revenue is primarily collected in the form of (i) Capitated revenue earned by providing healthcare service to Medicare Advantage attributed beneficiaries for a defined group of services including professional, institutional and pharmacy through a contract that is typically known as an “at-risk contract”, (ii) Shared savings earned based on improved quality and lower cost of care for our attributed lives in VBC incentive arrangements and (iii) Care management fees to cover costs of services typically not reimbursed under traditional FFS payment models, including population management, care coordination, advanced technology and analytics. VBC revenue represented 29.0%, 26.3% and 33.8% of total revenue for the years ended December 31, 2025, 2024, and 2023, respectively.
Other Revenue
The remainder of our revenue is derived from leveraging our existing base of providers and patients to deliver value-oriented services such as virtual visits, virtual scribes and coding. Other revenue represented 0.4% of total revenue for the years ended December 31, 2025 and 0.5% for the years ended December 31, 2024, and 2023, respectively.
Key Factors Affecting Our Performance
Addition of New Providers
Our ability to increase our provider base enables us to deliver financial growth as our providers generate both our FFS and VBC revenue. Our existing provider relationships and market share provides us with significant opportunity to grow in both existing and new geographies, and we believe the number of providers joining Privia is a key indicator of the market’s recognition of the attractiveness of our platform to our providers, patients and payers. We intend to increase our provider base in existing and new markets by adding new practices and assisting our existing practices with recruiting new providers, using our in-market and national sales and marketing teams. As we add providers to the Privia Platform, we expect them to contribute incremental economics as we leverage our existing brand and infrastructure, both at the corporate and in-market levels.
Addition of New Patients
Our ability to add new patients to our provider base in existing and new markets also enables us to deliver revenue growth in both our FFS and VBC contracts. We believe the number of attributed patient lives in VBC programs is a key driver of our VBC revenue growth. Our branding and marketing strategies to drive growth in our practices have continued to result in increased engagement with new and existing patients. We believe our continued success in growing the visibility of the Privia brand will result in increased patient panels per provider and contribute incremental revenue in both FFS and VBC for our practices.
Expansion to New Markets
Based upon our experience to date, we believe Privia can succeed in all reimbursement environments and payment models. The data we collected from older provider cohorts consistently suggest that we improve provider performance in both FFS and VBC metrics over time. It also informs our expectations for our new markets. We believe our in-market operating structure and ability to serve providers, wherever they are on their transition to VBC can benefit physicians and providers throughout the U.S. and that our solution is applicable across all 50 states. We enter a market with an asset-light operating model and employ a disciplined, uniform approach to market structure and development. We partner with market leading medical groups and health systems to form anchor relationships and align other independent, affiliated, or employed providers into a single-TIN medical group. Our business model also gives us flexibility for future, incremental growth through the acquisition of minority or majority stakes in our practices and opening de-novo, fully-owned sites of care focused on Medicare Advantage and direct contracting models.
During 2023, we entered four new markets through partnerships or affiliations with clinically integrated networks, health systems and independent group practices in Connecticut, Ohio, Washington state and South Carolina.
In November 2024, we announced it had entered into the Indiana market through the acquisition of an independent group practice, renamed Privia Medical Group Indiana, LLC (“PMG IN”), whereby Privia acquired majority ownership in PMG IN.
In April 2025, we announced a partnership with Integrated Medical Services, a multi-specialty practice, to launch Privia Medical Group Arizona (“PMG AZ”). Privia acquired a majority ownership in PMG AZ.
In December 2025, we acquired Evolent Health, Inc.’s accountable care business, adding over 120,000 attributed lives through the MSSP, as well as various commercial and Medicare Advantage programs.
Provider Satisfaction and Retention
Privia Providers have high satisfaction with their overall performance on our platform, and we strive to continuously improve provider well-being and patient satisfaction. Our percentage of collections model combined with high patient and provider satisfaction results in 90%+ Practice Collections predictability on a rolling twelve month forward basis. We believe these metrics demonstrate the stability of our provider base and the appeal to prospective providers and patients of our platform.
Payer Contracts and Ability to Move Markets to VBC
Our FFS and VBC revenue is dependent upon our contracts and relationships with payers. We partner with a large and varied set of payer groups nationally and in each of our markets to form provider networks and to lower the overall cost of care, and we structure bespoke contracts to help both providers and payers achieve their objectives in a mutually aligned manner. Maintaining, supporting and increasing the number of these contracts and relationships, particularly as we enter new markets, is important for our long-term success. We typically enter into multiyear contracts with our Medical Groups, Privia Physicians, health system or hospital partners, ACO participants and payer customers, which often have a stated initial term of three years with an automatic successive one-year renewal. From time to time, we may renegotiate or attempt to renegotiate our payer contracts in the ordinary course of business prior to the expiration of their stated terms. If the counterparties fail to renew their contracts, renew their contracts upon less favorable terms or at lower fee levels, fail to utilize additional products and services obtained from us, or if we fail to renegotiate contracts with our counterparties on favorable terms or at all, our revenue may decline and our future revenue growth may be constrained.
Our ability to work within each geographic market as it evolves in its shift towards VBC, with our experience working in all reimbursement environments, enables providers to accelerate and succeed in their transition. Our model is aligned with our payer partners, as we have demonstrated improved patient outcomes while driving incremental revenue growth. We intend to accelerate the move towards the adoption of VBC reimbursement in each market in current and emerging payer programs. To do so, we will need to continue enhancing our VBC capabilities and executing on initiatives to deliver next generation access, superior quality metrics and lower cost of care.
As of December 31, 2025, the total number of Privia-owned ACOs is ten.
During 2022 and 2023, we entered into capitated payer arrangements. Capitated revenue is generated through what is typically known as an “at-risk contract.” At-risk capitation refers to a model in which we are entitled to fixed monthly fees from the third-party payer in exchange for providing healthcare services to attributed beneficiaries in Medicare Advantage plans. The fees are typically based on a percentage of the defined premium that payers receive from CMS. We are responsible for providing or paying for the cost of healthcare services required by those attributed beneficiaries. At-risk capitated fees are recorded gross in revenues because we are acting as a principal in arranging for, providing, and controlling the managed healthcare services provided to the attributed beneficiaries. Given recent regulatory and utilization headwinds in Medicare Advantage, during the first quarter of 2024, we renegotiated certain capitation agreements for more favorable contract structures.
Components of Revenue
Our FFS revenue is primarily dependent upon the size of our provider base, payer contracted rates and patient volume. Our ability to maintain or improve pricing levels in our contracts with payers and patient volume for our providers will impact our results of operations. In addition to increasing our provider base and contracted rates over time, we also seek to increase patient volume by
demonstrating the ability to provide a better patient experience that leads to higher retention rates and drives referrals to preferred, high quality and value-based providers. Our VBC revenue is primarily dependent upon the number of attributed patients in our VBC arrangements, risk levels of our payer contracts, and effective management of our patients’ total cost of care. As we grow our provider base, we also expect to increase our total number of attributed patients in existing and new markets. In addition, we intend to increase the risk levels of our value-based programs as we seek a higher revenue opportunity on a per patient basis over time.
Investments in Growth
We expect to continue focusing on long-term growth through investments in our sales and marketing, our technology-enabled platform, and our operations. In addition, as we continue our efforts to move markets toward VBC, we expect to continue making additional investments in operations for an expanded suite of clinical capabilities to manage our patient population.
We launched Privia Care Partners on January 1, 2022 to offer a more flexible affiliation model for providers who do not desire to join one of our medical groups. This model aggregates providers in certain of our existing markets as well as new markets who are looking solely for VBC solutions without the necessity of changing EMR providers. We furnish population health services, reporting and analytics to such providers along with a menu of management services from which providers may choose. Since then, a number of Privia Care Partners’ providers transitioned to our Privia Medical Group model, which demonstrates the flexibility of our operating model and technology platform, as well as the ability to support physicians wherever they are in their transition value-based care.
Key Metrics and Non-GAAP Financial Measures
We review a number of operating and financial metrics, including the following key metrics and non-GAAP financial measures, to evaluate our business, measure our performance, identify trends affecting our business, formulate our business plans, and make strategic decisions.
Key Metrics | | | | | | | | | | | | | | | | | |
| For the Years Ended December 31, |
| 2025 | | 2024 | | 2023 |
| Implemented Providers (as of end of period) | 5,380 | | | 4,789 | | | 4,305 | |
Attributed Lives (in thousands) (as of end of period) | 1,541 | | | 1,256 | | | 1,120 | |
Practice Collections (1) ($ in millions) | $ | 3,470.5 | | | $ | 2,968.0 | | | $ | 2,839.0 | |
Implemented Providers
We define Implemented Providers as the total of all service professionals at the end of a given period who are credentialed and bill for medical services in both Owned and Non-Owned Medical Groups during that period. This includes, but is not limited to, physicians, physician assistants, and nurse practitioners. We believe that growth in the number of Implemented Providers is a key indicator of the performance of our business and expected revenue growth. This growth depends, in part, on our ability to successfully add new practices in existing markets and expand into new markets. The number of Implemented Providers increased 12.3% as of the year ended December 31, 2025, as compared to the year ended December 31, 2024, primarily due to organic growth in our healthcare delivery business as well as entrance into the Arizona market. Implemented Providers increased 11.2% as of the year ended December 31, 2024, compared to the year ended December 31, 2023, primarily due to organic growth in our healthcare delivery business as well as entrance into the Indiana market.
Attributed Lives
We define Attributed Lives as any patient that a payer deems attributed to Privia to deliver care as part of a value-based care arrangement through a provider of primary care services as of the end of a particular period. The number of Attributed Lives is an important measure that impacts the amount of VBC revenue we receive. Attributed Lives increased 22.7% as of December 31, 2025, compared to December 31, 2024 primarily due to acquisitions and organic growth. Attributed Lives increased 12.1% as of December 31, 2024, compared to December 31, 2023, primarily due to acquisitions and organic growth.
Practice Collections
We define Practice Collections as the total collections from all practices in all markets and all sources of reimbursement (FFS, VBC and other) that we receive for delivering care and providing our platform and associated services. Practice Collections differ from revenue by adding collections from Non-Owned Medical Groups both in FFS and VBC arrangements. FFS arrangements accounted for 81.6%, 83.2% and 76.5% of our Practice Collections for the years ended December 31, 2025, 2024, and 2023, respectively, while VBC accounted for 18.2%, 16.6% and 23.2% of Practice Collections for the years ended December 31, 2025, 2024, and 2023, respectively.
Practice Collections increased 16.9% for the year ended December 31, 2025 when compared with the same period in 2024 primarily due to organic growth of our healthcare delivery business and acquisitions. Practice Collections increased 4.5% for the year ended
December 31, 2024, compared with the same period in 2023, primarily due to organic growth of our healthcare delivery business and acquisitions.
Non-GAAP Financial Measures
In addition to our financial results determined in accordance with GAAP, we believe non-GAAP financial measures including Care Margin, Platform Contribution, Platform Contribution Margin, Adjusted EBITDA and Adjusted EBITDA Margin are useful measures to investors as these metrics are used by management in evaluating our operating performance and in assessing the health of our business. We use these non-GAAP measures to evaluate our ongoing operations and for internal planning and forecasting purposes. We believe that these non-GAAP financial measures, when taken together with the corresponding GAAP financial measures, provide meaningful supplemental information regarding our performance by excluding certain items that may not be indicative of our business, results of operations or outlook.
However, non-GAAP financial information is presented for supplemental informational purposes only, has limitations as an analytical tool and should not be considered in isolation or as a substitute for financial information presented in accordance with GAAP. In addition, other companies, including companies in our industry, may calculate similarly-titled non-GAAP measures differently or may use other measures to evaluate their performance, all of which could reduce the usefulness of our non-GAAP financial measure as a tool for comparison. Below is a reconciliation of our non-GAAP financial measures to the most directly comparable financial measure stated in accordance with GAAP. Investors are encouraged to review the related GAAP financial measures and the reconciliation of non-GAAP financial measures to their most directly comparable GAAP financial measures, and not to rely on any single financial measure to evaluate our business.
| | | | | | | | | | | | | | | | | |
| For the Years Ended December 31, |
(Dollars in thousands, except for percentages) | 2025 | | 2024 | | 2023 |
Care Margin 1 ($) | $ | 462,162 | | $ | 403,853 | | $ | 359,164 |
Platform Contribution 1 ($) | $ | 234,821 | | $ | 195,634 | | $ | 173,481 |
Platform Contribution Margin 1 (%) | 50.8% | | 48.4% | | 48.3% |
Adjusted EBITDA 1 ($) | $ | 125,549 | | $ | 90,455 | | $ | 72,228 |
Adjusted EBITDA Margin 1 (%) | 27.2% | | 22.4% | | 20.1% |
1. See below for more information as to how we define and calculate Care Margin, Platform Contribution, Platform Contribution Margin, Adjusted EBITDA and Adjusted EBITDA Margin and for a reconciliation of Gross Profit, the most comparable GAAP measure, to Care Margin, Gross Profit the most comparable GAAP measure, to Platform Contribution, and net income, the most comparable GAAP measure, to Adjusted EBITDA. |
Care Margin
Gross Profit is defined as total revenue less provider expenses and amortization of intangible assets. We define Care Margin as Gross Profit excluding amortization of intangible assets. Our Care Margin generated from FFS revenue is contractual and recurring in nature, and primarily based on an individually negotiated percentage of collections for each practice that joins Privia. Our Care Margin generated from VBC revenue is based on a percentage of care management fees and shared savings collected. We view Care Margin as all of the dollars available for us to manage our business, including providing administrative support to our practices, investing in sales and marketing to attract new providers to the Privia Platform, and supporting the organization through our corporate infrastructure. We expect Care Margin will grow year-over-year in absolute dollars as we continue to expand our provider base. We would also expect our care management and shared savings economics in our VBC arrangements to improve on a per patient basis as we manage towards lower total cost of care for our Attributed Lives and move towards higher risk VBC arrangements over time. Care Margin increased 14.4% for the year ended December 31, 2025 when compared to the same period in 2024 and increased 12.4% as of the year ended December 31, 2024, as compared to the same period in 2023, in each case due to organic growth of our medical practice business. As a percentage of revenue, Care Margin was 21.8% for the year ended December 31, 2025 a decrease from 23.3% for the same period in 2024. We continue to make strategic investments to increase services to both our patients and physicians. As a percentage of revenue, Care Margin was 23.3% in 2024 an increase from 21.7% in 2023, due to renegotiated certain at-risk capitation agreements for a more favorable contract structure which is reflected on a net basis under shared savings starting in 2024.
In addition to our financial results determined in accordance with GAAP, we believe Care Margin, a non-GAAP measure, is useful in evaluating our operating performance. We use Care Margin to evaluate our ongoing operations and for internal planning and forecasting purposes. We believe that this non-GAAP financial measure, when taken together with the corresponding GAAP financial measures, provides meaningful supplemental information regarding our performance by excluding certain items that may not be indicative of our business, results of operations or outlook. In particular, we believe that the use of Care Margin is helpful to our investors as it is a metric used by management in assessing the health of our business and our operating performance.
The following table provides a reconciliation of Gross Profit, exclusive of intangible asset amortization, the most closely comparable GAAP financial measure, to Care Margin:
| | | | | | | | | | | | | | | | | |
| For the Years Ended December 31, |
| (unaudited and amounts in thousands) | 2025 | | 2024 | | 2023 |
| Revenue | $ | 2,122,842 | | | $ | 1,736,390 | | | $ | 1,657,737 | |
| Provider expense | (1,660,680) | | | (1,332,537) | | | (1,298,573) | |
| Amortization of intangible assets | (9,168) | | | (6,164) | | | (5,359) | |
| Gross Profit | $ | 452,994 | | | $ | 397,689 | | | $ | 353,805 | |
| Amortization of intangible assets | 9,168 | | | 6,164 | | | 5,359 | |
| Care Margin | $ | 462,162 | | | $ | 403,853 | | | $ | 359,164 | |
Platform Contribution
We define Platform Contribution as Gross Profit, excluding amortization of intangible assets, less Cost of platform and excluding stock-based compensation expense included in Cost of platform. The following table provides a reconciliation of Gross Profit, the most closely comparable GAAP financial measure, to Platform Contribution. We consider Platform Contribution to be an important measure to monitor our performance, specific to pricing of our services, direct costs of delivering care, and cost of our platform and associated services. As a provider spends a longer time on the Privia Platform, we expect the Platform Contribution from that provider to increase both in terms of absolute dollars as well as a percent of Care Margin. We expect that this increase will be driven by improving per provider revenue economics over time as well as our ability to generate leverage on our in-market infrastructure costs. Platform Contribution increased 20.0% for the year ended December 31, 2025 when compared to the same period in 2024 and increased 12.8% between 2024 and 2023, in each case due to organic and inorganic growth of our medical practice business and a change in estimate related to our Shared Savings accrual.
The following table provides a reconciliation of Gross Profit, the most closely comparable GAAP financial measure, to Platform Contribution:
| | | | | | | | | | | | | | | | | |
| For the Years Ended December 31, |
| (unaudited and amounts in thousands) | 2025 | | 2024 | | 2023 |
| Revenue | $ | 2,122,842 | | | $ | 1,736,390 | | | $ | 1,657,737 | |
| Provider expense | (1,660,680) | | | (1,332,537) | | | (1,298,573) | |
| Amortization of intangible assets | (9,168) | | | (6,164) | | | (5,359) | |
| Gross Profit | $ | 452,994 | | | $ | 397,689 | | | $ | 353,805 | |
| Amortization of intangible assets | 9,168 | | | 6,164 | | | 5,359 | |
| Cost of platform | (252,732) | | | (227,000) | | | (197,663) | |
Stock-based compensation(1) | 25,391 | | | 18,781 | | | 11,980 | |
| Platform Contribution | $ | 234,821 | | | $ | 195,634 | | | $ | 173,481 | |
(1) Amount represents stock-based compensation expense included under Cost of platform. | | |
Platform Contribution Margin
We define Platform Contribution Margin as Platform Contribution as a percentage of Care Margin. We consider Platform Contribution Margin to be an important measure to monitor our performance, specific to pricing of our services, direct costs of delivering care, and cost of our platform and associated services. As a provider spends a longer time on the Privia Platform, we expect the Platform Contribution from that provider to increase both in terms of absolute dollars as well as a percent of Care Margin. We expect that this increase will be driven by improving per provider revenue economics over time as well as our ability to generate operating leverage on our in-market infrastructure costs. Platform Contribution Margin was 50.8% for the year ended December 31, 2025 compared with 48.4% during the same period in 2024 and 48.3% in 2023. We continue to make strategic investments intended to provide better service to both our patients and physicians at a pace slower than the increase in revenue.
In addition to our financial results determined in accordance with GAAP, we believe Platform Contribution and Platform Contribution Margin, each, a non-GAAP financial measure, are useful in evaluating our operating performance. We use Platform Contribution to evaluate our ongoing operations as well as for internal planning and forecasting purposes. We believe that these non-GAAP financial measures, when taken together with the corresponding GAAP financial measures, provide meaningful supplemental information regarding our performance by excluding certain items that may not be indicative of our business, results of operations or outlook. In particular, we believe that the use of Platform Contribution is helpful to our investors as they are metrics used by management in assessing the health of our business and our operating performance.
Adjusted EBITDA
We define Adjusted EBITDA as net income before interest income, net, provision for income taxes, net income (loss) attributable to non-controlling interests, depreciation and amortization, non-cash stock-based compensation, and other expenses including employer taxes on equity vesting and exercises and other certain non-recurring items such as severance, and other expenses. We include Adjusted EBITDA because it is an important measure by which we assess, and believe investors should assess, our operating performance. We consider Adjusted EBITDA to be an important measure because it helps illustrate underlying trends in our business and our historical operating performance on a more consistent basis. Adjusted EBITDA has limitations as an analytical tool as it: (i) does not reflect the impact of stock-based compensation expense, and (ii) does not reflect interest expense on our debt or the cash requirements necessary to service interest or principal payments, if any. Adjusted EBITDA increased 38.8% for the year ended December 31, 2025, as compared to the same period in 2024, and 25.2% for the year ended December 31, 2024, as compared to the same period in 2023, in each case due to organic and inorganic growth of our medical practice business and growth in Attributed Lives and a focus on managing the investment in new expenses.
Adjusted EBITDA Margin
We define Adjusted EBITDA Margin as Adjusted EBITDA as a percentage of Care Margin. We included Adjusted EBITDA Margin because it is an important measure on which we assess, and believe investors should assess, our operating performance. We consider Adjusted EBITDA Margin to be an important measure because it helps illustrate underlying trends in our business and our historical operating performance on a more consistent basis. Adjusted EBITDA Margin was 27.2%, 22.4%, and 20.1% for the years ended December 31, 2025, 2024, and 2023, respectively, in each case due to organic and inorganic growth of our medical practice business, growth in Attributed Lives and a focus on managing the investment in new expenses.
We believe that Adjusted EBITDA and Adjusted EBITDA Margin, when taken together with the corresponding GAAP financial measures, provide meaningful supplemental information regarding our performance by excluding certain items that may not be indicative of our business, results of operations or outlook. In particular, we believe that the use of Adjusted EBITDA and Adjusted EBITDA Margin is helpful to our investors as they are metrics used by management in assessing the health of our business and our operating performance.
The following table provides a reconciliation of net income attributable to the Company, the most closely comparable GAAP financial measure, to Adjusted EBITDA:
| | | | | | | | | | | | | | | | | |
| For the Years Ended December 31, |
| (unaudited and amounts in thousands) | 2025 | | 2024 | | 2023 |
| | | | | |
Net income attributable to Privia Health Group, Inc. | $ | 22,919 | | | $ | 14,385 | | | $ | 23,079 | |
Net income (loss) attributable to non-controlling interests | 6,807 | | | 2,659 | | | (2,051) | |
Provision for income taxes | 14,212 | | | 10,826 | | | 7,993 | |
Interest income, net | (9,703) | | | (10,888) | | | (8,372) | |
| Depreciation and amortization | 9,907 | | | 7,268 | | | 6,533 | |
| Stock-based compensation | 71,068 | | | 56,680 | | | 37,098 | |
Other expenses(1) | 10,339 | | | 9,525 | | | 7,948 | |
| Adjusted EBITDA | $ | 125,549 | | | $ | 90,455 | | | $ | 72,228 | |
| | | | | |
(1) Other expenses include employer taxes on equity vesting and exercises, severance and retention costs and certain other non-recurring costs. |
Components of Results of Operations
Revenue
As noted above under “Our Revenue,” revenue is earned in three main categories: FFS revenue, VBC revenue and other revenue.
Operating Expenses
Provider expenses
Provider expenses are amounts accrued or payments made to physicians, hospitals and other service providers, including Privia physicians, their related physician practices, and providers we have contracted with through payer partners. Those costs include physician guaranteed payments and other required distributions pursuant to the service agreements as well as medical claims costs for services provided to attributed beneficiaries under at-risk Capitated revenue arrangements for which we are financially responsible whether paid directly by us or indirectly by payers with whom we have contracted. Provider expenses are recognized in the period in which services are provided.
Cost of platform
Third-party EMR and practice management software expenses are paid on a percentage of revenue basis, while we pay most of the costs of our platform on a variable basis related to the number of implemented physicians we service. In addition, expenses contain stock-based compensation related to employees that provide Cost of platform services, but exclude any depreciation and amortization expense. As we continue to grow, we expect the cost of platform to continue to grow at a rate slower than the revenue growth rate.
Sales and marketing
Sales and marketing expenses consist of employee-related expenses, including salaries, commissions, stock-based compensation, and employee benefits costs, for all of our employees engaged in marketing, sales, community outreach, and sales support. In addition, sales and marketing expenses also include central and community-based advertising to generate greater awareness, engagement, and retention among our current and prospective patients as well as the infrastructure required to support all of our marketing efforts.
General and administrative
Corporate, general and administrative expenses include employee-related expenses, including salaries and related costs and stock-based compensation, technology infrastructure, occupancy costs, operations, clinical and quality support, finance, legal, human resources, and development departments.
Depreciation and amortization expense
Depreciation and amortization expenses consists of definitive-lived intangible asset amortization and depreciation of our fixed assets. We do not allocate depreciation and amortization expenses to other operating expense categories within our financial statements.
Interest income, net
Interest income consists primarily of interest earned by the Company on bank balances, partially offset by interest expense (including deferred financing costs) in connection with our borrowings. See “Liquidity and Capital Resources.”
Results of Operations
Year Ended December 31, 2025 Compared To Year Ended December 31, 2024
The following table sets forth our consolidated statements of operations data for the years ended December 31, 2025 and 2024. A detailed discussion of our 2023 financial condition and results of operations, and of 2024 year-over-year changes as compared to 2023, can be found in “Item 7—Management’s Discussion and Analysis of Financial Condition and Results of Operations” in our Annual Report on Form 10-K for the year ended December 31, 2024, which was filed with the SEC on February 27, 2025.
| | | | | | | | | | | | | | | | | | | | | | | | | | |
| | For the Years Ended December 31, | | | | |
| | 2025 | | 2024 | | Change ($) | | Change (%) |
| (in thousands) | | | | | | | | |
| Revenue | | $ | 2,122,842 | | | $ | 1,736,390 | | | $ | 386,452 | | | 22.3 | % |
| Operating expenses: | | | | | | | | |
| Provider expense | | 1,660,680 | | | 1,332,537 | | | 328,143 | | | 24.6 | % |
| Cost of platform | | 252,732 | | | 227,000 | | | 25,732 | | | 11.3 | % |
| Sales and marketing | | 27,136 | | | 26,446 | | | 690 | | | 2.6 | % |
| General and administrative | | 138,152 | | | 126,157 | | | 11,995 | | | 9.5 | % |
| Depreciation and amortization | | 9,907 | | | 7,268 | | | 2,639 | | | 36.3 | % |
| Total operating expenses | | 2,088,607 | | | 1,719,408 | | | 369,199 | | | 21.5 | % |
Operating income | | 34,235 | | | 16,982 | | | 17,253 | | | 101.6 | % |
| Interest income, net | | 9,703 | | | 10,888 | | | (1,185) | | | (10.9) | % |
Income before provision for income taxes | | 43,938 | | | 27,870 | | | 16,068 | | | 57.7 | % |
Provision for income taxes | | 14,212 | | | 10,826 | | | 3,386 | | | 31.3 | % |
Net income | | 29,726 | | | 17,044 | | | 12,682 | | | 74.4 | % |
Less: Net income attributable to non-controlling interests | | 6,807 | | | 2,659 | | | 4,148 | | | 156.0 | % |
Net income attributable to Privia Health Group, Inc. | | $ | 22,919 | | | $ | 14,385 | | | $ | 8,534 | | | 59.3 | % |
Revenue
The following table presents our revenues disaggregated by source:
| | | | | | | | | | | | | | | | | | | | | | | |
| For the Years Ended December 31, | | | | |
| (Dollars in Thousands) | 2025 | | 2024 | | Change ($) | | Change (%) |
| FFS-patient care | $ | 1,360,235 | | | $ | 1,146,156 | | | $ | 214,079 | | | 18.7 | % |
| FFS-administrative services | 137,017 | | | 125,431 | | | 11,586 | | | 9.2 | % |
| Capitated revenue | 308,458 | | | 212,987 | | | 95,471 | | | 44.8 | % |
| Shared savings | 234,815 | | | 179,202 | | | 55,613 | | | 31.0 | % |
| Care management fees (PMPM) | 73,138 | | | 64,066 | | | 9,072 | | | 14.2 | % |
| Other revenue | 9,179 | | | 8,548 | | | 631 | | | 7.4 | % |
| Total Revenue | $ | 2,122,842 | | | $ | 1,736,390 | | | $ | 386,452 | | | 22.3 | % |
Revenue was $2.12 billion for the year ended December 31, 2025, an increase from $1.74 billion for the year ended December 31, 2024. Key drivers of this revenue growth include: FFS–patient care revenue and FFS-administrative services, which increased $214.1 million and $11.6 million, primarily attributable to the addition of new providers and an increase in visit volume; an increase in capitated revenue of $95.5 million primarily due to an increase in Attributed Lives related to capitated arrangements, improved contract terms and an increase in estimated per capita revenue; shared savings revenue, which increased $55.6 million primarily due to more Attributed Lives in Medicare programs as well as continued strong estimated performance in our value based care programs in the aggregate; and an increase in PMPM revenue of $9.1 million primarily due to increased Attributed Lives.
Operating Expenses
| | | | | | | | | | | | | | | | | | | | | | | |
| For the Years Ended December 31, | | | | |
| (Dollars in Thousands) | 2025 | | 2024 | | Change ($) | | Change (%) |
| Operating Expenses: | | | | | | | |
| Provider expense | $ | 1,660,680 | | | $ | 1,332,537 | | | $ | 328,143 | | | 24.6 | % |
| Cost of platform | 252,732 | | | 227,000 | | | 25,732 | | | 11.3 | % |
| Sales and marketing | 27,136 | | | 26,446 | | | 690 | | | 2.6 | % |
| General and administrative | 138,152 | | | 126,157 | | | 11,995 | | | 9.5 | % |
| Depreciation and amortization expense | 9,907 | | | 7,268 | | | 2,639 | | | 36.3 | % |
| Total operating expenses | $ | 2,088,607 | | | $ | 1,719,408 | | | $ | 369,199 | | | 21.5 | % |
Provider expense
Provider expense was $1.66 billion for the year ended December 31, 2025, an increase from $1.33 billion during the same period in 2024. This increase was driven primarily by an increase in provider expenses associated with higher FFS-patient care revenue and growth in Implemented Providers.
Cost of platform
Cost of platform expense was $252.7 million for the year ended December 31, 2025, an increase from $227.0 million during the same period in 2024. The increase was driven by an increase in salaries and benefits of $11.4 million, an increase in stock-based compensation expense of $6.6 million, primarily related to an increase in stock-based awards granted in 2025 compared to 2024, and an increase of $6.1 million in professional services primarily due to continued growth in Implemented Providers and market expansion.
Sales and marketing
Sales and marketing expense was $27.1 million for the year ended December 31, 2025, an increase from $26.4 million during the same period in 2024. The increase was driven primarily by an increase in stock-based compensation expense of $1.3 million partially offset by immaterial cost reductions in other sales and marketing expenses.
General and administrative
General and administrative expenses were $138.2 million for the year ended December 31, 2025, an increase from $126.2 million during the same period in 2024. The increase was driven by the increase of $6.5 million in stock-based compensation expense, an increase in salaries and benefits of $3.6 million and an increase in professional services of $2.4 million related to additional consulting services.
Depreciation and amortization expense
Depreciation and amortization expenses were $9.9 million for the year ended December 31, 2025, compared to $7.3 million during the same period in 2024. This increase was primarily driven by definitive-lived intangible asset amortization associated with business combinations.
Interest income, net
Interest income, net was $9.7 million for the year ended December 31, 2025, compared to $10.9 million during the same period in 2024 primarily driven by lower cash and cash equivalents during the comparative periods. Interest income is primarily based on the cash balance held in interest bearing accounts.
Provision for income taxes
The provision for income taxes was $14.2 million for the year ended December 31, 2025, compared to $10.8 million during the comparative period in 2024. The provision for income taxes increased as a result of higher income before income taxes.
Net income attributable to non-controlling interests
Net income attributable to non-controlling interests was $6.8 million for the year ended December 31, 2025, an increase compared to $2.7 million during the comparative period in 2024. The change is primarily related to continued growth in existing markets.
Liquidity and Capital Resources
General
To date, we have financed our operations principally through sale of our equity, payments received from various payers and through borrowings under the Credit Facilities. As of December 31, 2025, we had cash and cash equivalents of $479.7 million. Our cash and cash equivalents primarily consist of highly liquid investments in money market funds and cash.
We believe that our cash and cash equivalents, together with cash flows from operations, will provide adequate resources to fund our short-term and long-term operating and capital needs. Our assessment of the period of time through which our financial resources will be adequate to support our operations is a forward-looking statement and involves risks and uncertainties. Our actual results could vary because of, and our future capital requirements will depend on many factors, including growth rate, and the timing and extent of spending to increase our sales and marketing activities. We may in the future enter into arrangements to acquire or invest in complementary businesses, services and technologies, including intellectual property rights. We have based this estimate on assumptions that may prove to be wrong, and we could use our available capital resources sooner than we currently expect. We may in the future seek funding for long-term capital structure flexibility, and may be required to seek additional equity or debt financing. In the event that additional financing is required from outside sources, we may not be able to raise it on terms acceptable to us or at all. If we are unable to raise additional capital when desired, or if we cannot expand our operations or otherwise capitalize on our business opportunities because we lack sufficient capital, our business, results of operations, and financial condition may be adversely affected.
Indebtedness
See Note 9. “Debt” for discussion on our Credit Facilities.
Cash Flows Overview
Our cash requirements within the next twelve months include provider liabilities, accounts payable and accrued liabilities, purchase commitments and other obligations. We expect the cash required to meet these obligations to be generated primarily through cash flows from current operations; cash available for general corporate use; and the realization of current assets, such as accounts receivable. Based on current and anticipated levels of operations, we believe that cash provided by operating activities, together with the available cash on hand at December 31, 2025, will be sufficient to meet anticipated cash requirements for both the short term (next 12 months) and long term (beyond 12 months).
The following table presents a summary of our consolidated cash flows from operating, investing and financing activities for the periods indicated:
| | | | | | | | | | | | | | | | | |
| For the Years Ended December 31, |
| 2025 | | 2024 | | 2023 |
| (in thousands) | | | | | |
Consolidated Statements of Cash Flows Data: | | | | | |
| Net cash provided by operating activities | $ | 163,404 | | | $ | 109,282 | | | $ | 80,785 | |
| Net cash used in investing activities | (181,570) | | | (11,978) | | | (42,971) | |
| Net cash provided by financing activities | 6,702 | | | 4,334 | | | 3,705 | |
| Net (decrease) increase in cash and cash equivalents | $ | (11,464) | | | $ | 101,638 | | | $ | 41,519 | |
Operating Activities
Net cash provided by operating activities was $163.4 million for the year ended December 31, 2025 compared to $109.3 million for the comparative period in 2024 primarily as a result of:
•An increase in net income of $12.7 million compared to the same period in 2024. Net income was $29.7 million during the year ended December 31, 2025 compared to the income of $17.0 million during the year ended December 31, 2024.
•An increase of $65.6 million in Provider Liability during the year ended December 31, 2025 compared to an increase of $32.9 million during the same period in 2024, a difference of $32.7 million. The increase is primarily due to an increase in Implemented Providers and an increase in provider expenses related to the increase in FFS and VBC revenue.
•An increase of $38.3 million in accounts receivable and prepaid and other current assets for the year ended December 31, 2025 compared to the same period in 2024 of $28.8 million, a difference of $9.5 million. The change is primarily due to an increase in FFS and VBC revenue.
Investing Activities
Net cash used in investing activities was $181.6 million for the year ended December 31, 2025 compared to $12.0 million during the same period in 2024, primarily due to business acquisitions in 2025.
Financing Activities
Net cash provided by financing activities was $6.7 million for the year ended December 31, 2025, compared to $4.3 million for the same period in 2024. This increase is primarily due to an increase in proceeds from stock options exercised during the year ended December 31, 2025.
Comparison of Fiscal 2024 to Fiscal 2023
A detailed discussion of our 2023 to 2024 operations and liquidity and capital resources has been omitted from this Form 10-K, but may be found in “Item 7—Management’s Discussion and Analysis of Financial Condition and Results of Operations” in our Annual Report on Form 10-K for the year ended December 31, 2024, which was filed with the SEC on February 27, 2025.
Contractual Obligations, Commitments and Contingencies
Operating Leases. We lease office space under various operating lease agreements. The initial terms of these leases range from 3 to 9 years and generally provide for periodic rent increases, renewal, and termination operations. Total rent expense under operating leases was $3.2 million for the year ended December 31, 2025, $2.8 million for the year ended December 31, 2024, and $2.7 million for the year ended December 31, 2023.
Off Balance Sheet Obligations. We do not have any off-balance sheet arrangements as of December 31, 2025.
Commitments and Contingencies. See Note 13. “Commitments and Contingencies” for further discussion on our commitments and contingencies.
Critical Accounting Policies and Estimates
Our consolidated financial statements have been prepared in accordance with U.S. GAAP. The preparation of these consolidated financial statements requires us to make estimates and assumptions that affect the reported amounts of assets, liabilities, revenue, expenses, and related disclosures. We base our estimates on historical experience and on various other factors that we believe are reasonable under the circumstances which we evaluate on an ongoing basis. Actual results may differ from these estimates. To the extent that there are material differences between these estimates and our actual results, our future financial statements will be affected.
While our significant accounting policies are described in greater detail in Note 1. “Organization and Summary of Significant Accounting Policies,” to our consolidated financial statements included elsewhere in this Annual Report, we believe that the following accounting policies are those most critical to the judgments and estimates used in the preparation of our consolidated financial statements.
Business Combinations
Accounting for business combinations requires us to allocate the fair value of purchase considerations to the tangible assets acquired, liabilities assumed, and intangible assets acquired based on their estimated fair values, which were determined primarily using the income method. The excess of the fair value of purchase consideration over the fair values of these identified assets and liabilities is recorded as goodwill. Such valuations require us to make significant estimates and assumptions, especially at the acquisition date with respect to intangible assets. Significant estimates in valuing certain intangible assets include, but are not limited to, revenue growth and attrition rates, medical claims expense, cost of care expenses, operating expenses, discount rate, contract terms and useful life from acquired assets.
Our estimates of fair value are based upon assumptions believed to be reasonable, but which are inherently uncertain and unpredictable and, as a result, actual results may differ from estimates. Allocation of purchase consideration to identifiable assets and liabilities affects our amortization expense, as acquired finite-lived intangible assets are amortized over the useful life, whereas any indefinite lived intangible assets, including goodwill, are not amortized. During the measurement period, which is not to exceed one year from the acquisition date, we may record adjustments to the assets acquired and liabilities assumed, with the corresponding offset to goodwill. Upon the conclusion of the measurement period, any subsequent adjustments are recorded to earnings. For additional details, refer to Note 3. “Business Combinations.”
Revenue Recognition
Revenue is recognized when a customer obtains control of promised goods or services, in an amount that reflects the consideration which the entity expects to receive in exchange for those goods or services. Revenue recognition is determined through the following five steps:
i.Identify the contract(s) with a customer;
ii.Identify the performance obligations in the contract;
iii.Determine the transaction price;
iv.Allocate the transaction price to the performance obligations in the contract; and
v.Recognize revenue as the entity satisfies a performance obligation.
FFS revenue
FFS-patient care
Our FFS-patient care revenue is generated primarily from providing healthcare services to patients. Providing medical services to patients represents our performance obligation under third-party payer agreements, and accordingly, the transaction price is allocated entirely to that one performance obligation. We recognize revenue as services are rendered and approved by the Privia Providers, which is typically a single day for each service. We receive payment for services from third-party payers, as well as from patients who have health insurance, but are also financially responsible for some or all of the service in the form of co-pays, coinsurance or deductibles. Patients who do not have health insurance are required to pay for their services in full.
FFS-patient care revenue is reported net of provisions for contractual allowances from third-party payers and patients. We have certain agreements with third-party payers that provide for reimbursement at amounts different from our standard billing rates. The differences between the estimated reimbursement rates and the standard billing rates are accounted for as contractual adjustments, which are deducted from gross revenue to arrive at FFS-patient care revenue. We determine our estimate of implicit price concessions based on our historical collection experience with classes of patients using a portfolio approach as a practical expedient to account for patient contracts as collective groups rather than individually. The financial statement effects of using this practical expedient are not materially different from an individual contract approach. Subsequent changes to the estimate of the transaction price (determined on a portfolio basis when applicable) are generally recorded as adjustments to revenue in the period of the change. For the years ended December 31, 2025, 2024, and 2023, changes in our estimates of implicit price concessions and contractual adjustments to expected payments for performance obligations satisfied in prior periods were not significant.
FFS-administrative services
The Company’s FFS-administrative services business provides administration and management services pursuant to MSAs with Non-Owned Medical Groups.
The Company’s MSAs with the Non-Owned Medical Groups range from 5 –20 years in duration and outline the terms and conditions of the administration and management services to be provided, which includes RCM services such as billings and collections, as well as other services, including, but not limited to, payer contracting, information technology services and accounting and treasury services.
In certain MSAs, the Company is paid administrative fees equal to the cost of supplying certain services as outlined in the MSAs, and if applicable, a margin is added to the cost of certain services. The margin, if applicable, is fixed based on the MSAs; however, the cost of supplying certain services can fluctuate during the life of the MSAs.
In certain MSAs, the Company is paid a percentage of net collections. The percentage is fixed per the MSAs; however, the net collections can fluctuate during the life of the contract.
Under each MSA, there is a single performance obligation to provide a series of administration and management services required for the contract period. The Company believes that each Non-Owned Medical Group receives the management and administrative services each day and has concluded that an output method is appropriate for recognizing administrative services revenue.
Administrative fees are reported at the amount that reflects the consideration to which the Company expects to be entitled in exchange for the provision of administration and management services to Non-Owned Medical Groups. In addition, certain of our MSAs include
rebates to the customers in the event that certain conditions occur. The Company estimates the transaction price using the most likely amount methodology and amounts are included in the net transaction price to the extent that it is probable that a significant reversal will not occur once any uncertainty associated with the variable consideration is subsequently resolved. Rebates of $3.5 million have been recorded for the years ended December 31, 2025, $1.8 million for the year ended December 31, 2024 and $2.7 million for the year ended December 31, 2023, respectively.
VBC revenue
The Company’s VBC business consists of its clinically integrated networks and ACOs which bring together independent physician practices within our medical groups to focus on sharing data, improving care coordination, and collaborating on initiatives to improve outcomes and lower healthcare spending. The Company has contracts with the U.S. federal government and large payer organizations that are multi-year in nature typically ranging from three to five years and is earned as follows: (1) Capitated revenue (2) on a shared savings basis and (3) Care management fees on a per member per month basis.
Capitated Revenue
Capitated revenue consists of capitation fees earned under contracts with various Medicare Advantage payers (“Payers”) in at-risk capitation arrangements. The Company is entitled to monthly fees to provide a defined range of healthcare services for Medicare Advantage health plan members (“attributed beneficiaries” or “attributed lives”) attributed to the Company’s contracted physicians (typically primary care). Monthly fees are determined as a percentage of the premium payers receive from CMS for these attributed beneficiaries. In at-risk arrangements, the Company generally accepts financial risk for beneficiaries attributed to its contracted physicians and, therefore, is responsible for the cost of contracted healthcare services required by those beneficiaries in accordance with the terms of each agreement. Fees are recorded gross in revenue because the Company is acting as a principal in coordinating and controlling the range of services provided (other than clinical decisions) under its Capitated revenue contracts with payers. Capitated revenue contracts with payers are generally multi-year arrangements and have a single monthly stand ready performance obligation, as defined by ASC Topic 606, Revenue from Contracts with Customers (“ASC 606”), to provide all aspects of necessary medical care to members for the contracted period. The Company recognizes revenue in the month in which the eligible beneficiary is entitled to receive healthcare benefits during the contract term.
The transaction price for the Company’s capitation contracts is a fixed percentage of premium per attributed life with periodic adjustment, as the monthly fees to which the Company are entitled are subject to periodic adjustments under CMS’s risk adjustment payment methodology. CMS deploys a risk adjustment model that determines premiums paid to all payers according to each attributed life’s health status and certain demographic factors. Under this risk adjustment methodology, CMS calculates the risk adjusted premium payment using diagnosis data from various settings. The Company and healthcare providers collect and submit diagnosis data to payers (and ultimately to CMS) to be utilized in the determination of risk adjustments and such data is used by the Company to estimate any adjustments to the Capitated revenue earned that may increase or decrease revenue in subsequent periods pursuant to contractual terms. Such adjustments are estimated using the most likely amount methodology and amounts are only included in revenue to the extent that it is probable that a significant reversal of cumulative revenue will not occur once any uncertainty is resolved. Capitated revenue fees are also subject to adjustment for incentives or penalties based on the achievement of certain quality metrics defined in the Company’s contracts with payers. The Company recognizes incentive revenue as earned using the most likely amount methodology and only to the extent that it is probable that a significant reversal of cumulative revenue will not occur once any uncertainty is resolved.
Neither the Company nor any of its affiliates are a registered insurance company as state law in the states in which we operate do not require such registration for risk bearing providers.
Shared Savings
Under the shared savings basis, the Company may earn financial incentives for increasing accountability over the cost, quality and efficiency of the care provided to attributed members. Incentive payments are earned when, for a given twelve-month measurement period, the Company meets or exceeds quality and utilization standards established by the payer and achieves savings on medical costs for the population of attributed members. To determine the amount of shared savings payments, payers evaluate the Company’s performance during the measurement period using the agreed-upon benchmarks, metrics and performance criteria.
The Company estimates the transaction price by analyzing performance during the relevant time period in connection with the contractually defined benchmarks, metrics, performance criteria, inflation trends, risk adjustment factors, attribution criteria and other factors. Revenue is recognized only when the price can be reasonably estimated and it is probable that a significant reversal will not occur once any uncertainty associated with the variable consideration is subsequently resolved. Shared savings revenue is recorded in the period under which when the underlying services are provided during the pre-set twelve-month measurement period.
Care Management Fees (“PMPM”)
Under the PMPM basis, the Company is paid a PMPM rate for each covered individual who is attributed by the payer to the Company (“attributed members”). The Company records revenue in the month for which the PMPM rate applies and the member was attributed.
The PMPM rate is based on a predetermined monthly contractual rate for each attributed member regardless of the volume of care coordination services provided under the contracts with the payers. The PMPM rate varies based on payer and product.
Revenue is reported at the amount that reflects the consideration to which the Company expects to be entitled in exchange for the provision of care coordination services to its population of attributed members. The Company’s contracts with payers have a single performance obligation that consists of a series of services for the provision of care coordination services for the population of attributed members for the duration of the contract. The transaction price for the contracts is entirely variable, as it is primarily based on a PMPM rate on monthly attributed membership, which can fluctuate during the life of the contract.
The majority of the Company’s net PMPM transaction price relates specifically to its efforts to transfer the service for a distinct increment of the series and is recognized as revenue in the month in which attributed members are entitled to care coordination services.
Other Revenue
The remainder of our revenue is derived from leveraging our existing base of providers and patients to deliver value-oriented services such as concierge services, virtual visits, virtual scribes and coding, clinical trials, behavioral health management, and partnerships with self-insured employers to offer direct primary care to their employees.
Provider Liability
Provider Liability represents costs payable to physicians, hospitals and other ancillary providers, including both Privia Physicians, their related practices, and providers the Company has contracted with through payer partners. Those costs include amounts that have not yet been paid for physician guaranteed payments and other required distributions pursuant to the service agreements as well as medical claims costs for services provided to attributed beneficiaries for which the Company is financially responsible under at-risk capitated revenue arrangements whether paid directly by the Company or indirectly by payers with whom the Company has contracted.
Stock-Based Compensation
The Company accounts for share-based compensation in accordance with the expense recognition provisions of ASC 718, Compensation–Stock Compensation (“ASC 718”), which requires the issuer to recognize compensation expense for all share-based payments made to employees based on the fair value of the share-based payment at the date of grant. Up until April 2021, the estimated fair value of share-based payments granted to the Company’s employees was determined using the Monte-Carlo option pricing model, which requires inputs based on certain subjective assumptions, including expected term of the option, expected stock price volatility, the risk free interest rate for a period that approximates the expected term of the option and the Company’s expected dividend yield (See Note 11. “Stockholders’ Equity”). The share-based payments granted or modified prior to April 2021 to employees of the Company do not have quoted market prices, and changes in subjective input assumptions can materially affect the fair value estimate. Since April 2021, the Company has estimated the fair value of the options granted to Company’s employees and contractors using the Black-Scholes option-pricing model. Option valuation models require several inputs, such as the expected stock price volatility, the fair value of the stock, the risk free rate, the expected term of the award and the dividend yield. The Company records share-based compensation forfeitures as a reversal of previously recognized compensation expense as the forfeitures occur. For additional details refer to Note 11. “Stockholders’ Equity.”
The Company issues certain performance stock units ("PSUs"). The awards will vest based on the satisfaction of certain service conditions, performance-based conditions, and market conditions. The Company has identified certain performance metrics associated with these awards that are measured on a cumulative basis over a three-year performance period. The targets for the first year of the PSU performance period are established at the time of grant. Targets for subsequent years’ PSU performance periods are set annually concurrently with granting and establishing the targets for subsequent years’ PSU grants. The Company has determined that the service inception date precedes the grant date for these awards as (a) the awards were authorized prior to establishing an accounting grant date, (b) the recipients began providing services prior to the grant date, and (c) there are performance conditions that, if not met by the accounting grant date, will result in the forfeiture of the awards. As the service inception date precedes the accounting grant date, the Company recognizes stock-based compensation expense over the requisite service period based on the estimated fair value at each reporting date.
ITEM 7A. QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK
Market risk represents the risk of loss that may impact our financial position due to adverse changes in financial market prices and rates. Our market risk exposure is primarily a result of exposure due to potential changes in inflation or interest rates. We do not hold financial instruments for trading purposes.
Interest Rate Risk
Our primary market risk exposure is rising interest rates. Interest rate risk is highly sensitive due to many factors, including U.S. monetary and tax policies, U.S. and international economic factors and other factors beyond our control. Our Credit Agreement bears interest at a base rate plus applicable margin ranging from 0.25% to 0.75%, or ii) Secured Overnight Financing Rate (“SOFR”) plus 0.10% plus an applicable margin ranging from 1.25% to 1.75% depending on the consolidated leverage ratio, as defined. In no event will the base rate be less than 1.0%. As of December 31, 2025, the Company had no outstanding debt under the Credit Agreement.
Inflation Risk
Based on our analysis of the periods presented, we believe that inflation has not had a material effect on our operating results. There can be no assurance that future inflation will not have an adverse impact on our operating results and financial condition.
ITEM 8. FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA
All information required by this item is included in Item 15 of this Annual Report on Form 10-K and is incorporated into this item by reference.
ITEM 9. CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURE
None.
ITEM 9A. CONTROLS AND PROCEDURES
Evaluation of Disclosure Controls and Procedures
Under the supervision and with the participation of our management, including the Chief Executive Officer and Chief Financial Officer, we have evaluated the effectiveness of our disclosure controls and procedures (as defined in Rules 13a-15(e) and 15d-15(e) under the Exchange Act), as of the end of the period covered by this report. Based on that evaluation, the Chief Executive Officer and Chief Financial Officer have concluded that these disclosure controls and procedures were effective at the reasonable assurance level as of December 31, 2025.
Management’s Annual Report on Internal Control Over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over financial reporting, as defined in Rules 13a-15(f) and 15d-15(f) under the Exchange Act. Our management, including our Chief Executive Officer and Chief Financial Officer, has evaluated the effectiveness of our internal control over financial reporting as of December 31, 2025. In assessing the effectiveness of our internal control over financial reporting, our management used the framework established in Internal Control Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission (“COSO”). Based on that evaluation, our management has concluded that our internal control over financial reporting was effective as of December 31, 2025.
The effectiveness of our internal control over financial reporting as of December 31, 2025, has been audited by PricewaterhouseCoopers LLP, an independent registered public accounting firm, as stated in their report, which can be found under Part IV of this Annual Report on Form 10-K.
Changes to our Internal Controls over Financial Reporting
There were no changes made to the Company’s internal control over financial reporting during the quarter ended December 31, 2025 that have materially affected, or are reasonably likely to materially affect, the Company’s internal control over financial reporting.
Inherent Limitation on the Effectiveness of Controls
The effectiveness of any system of internal control over financial reporting, including ours, is subject to inherent limitations, including the exercise of judgment in designing, implementing, operating, and evaluating the controls and procedures, and the inability to eliminate misconduct completely. Accordingly, in designing and evaluating the disclosure controls and procedures, management recognizes that any system of internal control over financial reporting, including ours, no matter how well designed and operated, can only provide reasonable, not absolute assurance of achieving the desired control objectives. In addition, the design of disclosure controls and procedures must reflect the fact that there are resource constraints and that management is required to apply its judgment in evaluating the benefits of possible controls and procedures relative to their costs. Moreover, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate. We intend to continue to monitor and upgrade our internal controls as necessary or appropriate for our business but cannot assure you that such improvements will be sufficient to provide us with effective internal control over financial reporting.
ITEM 9B. OTHER INFORMATION
During the fourth quarter of 2025, no director or officer (as defined in Rule 16a-1(f) under the Exchange Act) of the Company adopted or terminated any Rule 10b5-1 trading arrangements or non-Rule 10b5-1 trading arrangements (in each case, as defined in Item 408(a) of Regulation S-K).
ITEM 9C. DISCLOSURE REGARDING FOREIGN JURISDICTION THAT PREVENT INSPECTIONS.
Not Applicable.
PART III
ITEM 10. DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE
We adopted a written Code of Ethics and business conduct that applies to our directors, executive officers and employees, including our Chief Executive Officer, President and Chief Operating Officer, General Counsel, Chief Financial Officer, principal accounting officer, the controller and all persons performing similar functions. A current copy of the code is posted under “Governance” on the Investor Relations section of our website, our website, ir.priviahealth.com. Any waiver from the Code of Ethics and any amendments to the Code of Ethics will be disclosed on such page of the Company’s website. Additionally, we have an insider trading policy governing the purchase, sale and other dispositions of the Company’s securities that applies to all of the Company’s directors, officers, employees and certain other covered individuals. The Company does not currently purchase its own securities through a share repurchase program, and we expect that any share repurchase program that may in the future be adopted by the Company would be subject to specific policies and procedures. The Company believes that its insider trading policy and procedures are reasonably designed to promote compliance with insider trading laws, rules, regulations and listing standards applicable to the Company. A copy of the Company’s insider trading policy is incorporated by reference as Exhibit 19.1 to this Annual Report on Form 10-K.
The additional information required by this item will be set forth in the definitive proxy statement to be filed with the SEC in connection with the Annual Meeting of Stockholders within 120 days after December 31, 2025 (the “Proxy Statement”) and is incorporated into this Annual Report on Form 10-K by reference.
ITEM 11. EXECUTIVE COMPENSATION
The information required by this item will be set forth in the Proxy Statement and is incorporated into this Annual Report on Form 10-K by reference.
ITEM 12. SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNER AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS
The information required by this item will be set forth in the Proxy Statement and is incorporated into this Annual Report on Form 10-K by reference.
ITEM 13. CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS, AND DIRECTOR INDEPENDENCE
The information required by this item will be set forth in the Proxy Statement and is incorporated into this Annual Report on Form 10-K by reference.
ITEM 14. PRINCIPAL ACCOUNTING FEES AND SERVICES
The information required by this item will be set forth in the Proxy Statement and is incorporated into this Annual Report on Form 10-K by reference.
PART IV
ITEM 15. Exhibits, Financial Statement Schedules.
(a)The following documents are filed as part of this Annual Report on Form 10- K:
1.Financial Statements:
The accompanying Index to Consolidated Financial Statements on page F-1 of this annual report on Form 10-K is provided in response to this item.
2.Financial Statement Schedules
None.
(b)Exhibits
The exhibits listed in the following “Exhibit Index” are filed, furnished or incorporated by reference as part of this Annual Report on Form 10-K.
ITEM 15. EXHIBITS
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
Exhibit
Number | | Description | | Form | | Exhibit | | File No. | | Filing Date | | Filed Herewith |
| | | | | | | | | | | | |
3.1+ | | | | 8-K | | 3.1 | | 001-40365 | | 05/23/2024 | | |
| | | | | | | | | | | | |
3.2+ | | | | 8-K | | 3.2 | | 001-40365 | | 05/23/2024 | | |
| | | | | | | | | | | | |
| 4.1+ | | | | S-1 | | 4.1 | | 333-255086 | | 04/07/2021 | | |
| | | | | | | | | | | | |
| 4.2+ | | | | 10-K | | 4.1 | | 001-40365 | | 11/06/2025 | | |
| | | | | | | | | | | | |
10.1+§ | | | | S-8 | | 99.1 | |
333-255598 | | 04/29/2021 | | |
| | | | | | | | | | | | |
10.2+§ | | | | S-1 | | 10.8+ | | 333-255086 | | 04/22/2021 | | |
| | | | | | | | | | | | |
10.3+§ | | | | S-1 | | 10.9+ | | 333-255086 | | 04/22/2021 | | |
| | | | | | | | | | | | |
10.4+§ | | | | S-1 | | 10.1 | | 333-255086 | | 04/22/2021 | | |
| | | | | | | | | | | | |
10.5+§ | | | | 10-K | | 10.35 | | 001-40365 | | 02/27/2025 | | |
| | | | | | | | | | | | |
10.6+§ | | | | S-1 | | 10.3 | | 333-255086 | | 04/07/2021 | | |
| | | | | | | | | | | | |
10.7+§ | | | | 10-Q | | 10.4 | | 221-155713 | | 08/11/2022 | | |
| | | | | | | | | | | | |
10.8+§ | | | | 10-K | | 10.4 | | 227-68304 | | 03/25/2022 | | |
| | | | | | | | | | | | |
10.9+§ | | | | 10-Q | | 10.5 | | 221-155713 | | 08/11/2022 | | |
| | | | | | | | | | | | |
| 10.10+§ | | | | 10-Q | | 10.6 | | 221-155713 | | 08/11/2022 | | |
| | | | | | | | | | | | |
10.11+§ | | | | 8-K | | 10.1 | | 001-40365 | | 06/29/2023 | | |
| | | | | | | | | | | | |
10.12+§ | | | | 8-K | | 10.1 | | 001-40365 | | 03/07/2025 | | |
| | | | | | | | | | | | |
10.13+§ | | | | 8-K | | 10.2 | | 001-40365 | | 03/22/2022 | | |
| | | | | | | | | | | | |
10.14+§ | | | | 10-Q | | 10.7 | | 221-155713 | | 08/11/2022 | | |
| | | | | | | | | | | | |
10.15+§ | | | | 10-Q | | 10.2 | | 001-40365 | | 05/08/2025 | | |
| | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
10.16+§ | | | | 10-K | | 10.1 | | 001-40365 | | 02/27/2024 | | |
| | | | | | | | | | | | |
10.17+§ | | | | 10-Q | | 10.3 | | 001-40365 | | 05/08/2025 | | |
| | | | | | | | | | | | |
10.18+ | | | | 8-K | | 10.1+ | | 001-40365 | | 05/03/2021 | | |
| | | | | | | | | | | | |
10.19+ | | | | 10-Q | | 10.11 | | 211-388036 | | 11/08/2021 | | |
| | | | | | | | | | | | |
10.20+§ | | | | S-1 | | 10.7+ | | 333-255086 | | 04/22/2021 | | |
| | | | | | | | | | | | |
10.21+§ | | | | S-8 | | 99.2 | | 333-255598 | | 04/29/2021 | | |
| | | | | | | | | | | | |
10.22+§ | | | | S-8 | | 99.3 | | 333-255598 | | 04/29/2021 | | |
| | | | | | | | | | | | |
10.23+§ | | | | S-8 | | 99.4 | | 333-255598 | | 04/29/2021 | | |
| | | | | | | | | | | | |
10.24+ | | | | 10-K | | 10.23 | | 227-68304 | | 03/25/2022 | | |
| | | | | | | | | | | | |
10.25+§ | | | | 10-Q | | 10.2 | | 001-40365 | | 05/04/2023 | | |
| | | | | | | | | | | | |
10.26+§ | | | | 10-Q | | 10.1 | | 001-40365 | | 05/04/2023 | | |
| | | | | | | | | | | | |
10.27+§ | | | | 8-K | | 10.2 | | 001-40365 | | 06/29/2023 | | |
| | | | | | | | | | | | |
10.28+ | | Credit Agreement dated as of November 16, 2023 among Privia Health Group, Inc., PH Group Holdings Corp., and Privia Health, LLC, as borrower, with Wells Fargo Bank, National Association, as issuing lender, and certain other lenders | | 8-K | | 10.1 | | 001-40365 | | 11/21/2023 | | |
| | | | | | | | | | | | |
10.29+§ | | | | 10-Q | | 10.1 | | 001-40365 | | 08/07/2025 | | |
| | | | | | | | | | | | |
10.30+§ | | | | | | | | | | | | X |
| | | | | | | | | | | | |
10.31+§ | | | | S-1 | | 10.4+ | | 333-255086 | | 04/07/2021 | | |
| | | | | | | | | | | | |
10.32+§ | | | | 10-K | | 10.6 | | 22768304 | | 03/25/2022 | | |
| | | | | | | | | | | | |
10.33+§ | | | | 10-K | | 10.7 | | 227-68304 | | 03/25/2022 | | |
| | | | | | | | | | | | |
10.34+§ | | | | 10-K | | 10.8 | | 227-68304 | | 03/25/2022 | | |
| | | | | | | | | | | | |
10.35+§ | | | | 10-Q | | 10.8 | | 221-155713 | | 08/11/2022 | | |
| | | | | | | | | | | | |
10.36+§ | | | | 8-K | | 10.1 | | 001-40365 | | 01/29/2024 | | |
| | | | | | | | | | | | |
| | | | | | | | | | | | |
| | | | | | | | | | | | |
| 19.1 | | | | 10-K | | 19.1 | | 001-40365 | | 02/27/2025 | | |
| | | | | | | | | | | | |
| 21.1 | | | | | | | | | | | | X |
| | | | | | | | | | | | |
| 23.1 | | | | | | | | | | | | X |
| | | | | | | | | | | | |
| 31.1 | | | | | | | | | | | | X |
| | | | | | | | | | | | |
| 31.2 | | | | | | | | | | | | X |
| | | | | | | | | | | | |
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| 32.1* | | | | | | | | | | | | X |
| | | | | | | | | | | | |
| 32.2* | | | | | | | | | | | | X |
| | | | | | | | | | | | |
| 97.1 | | | | 10-K | | 97.1 | | 001-40365 | | 02/27/2024 | | |
| | | | | | | | | | | | |
| 101.INS | | XBRL Instance Document ** | | | | | | | | | | X |
| | | | | | | | | | | | |
| 101.SCH | | XBRL Taxonomy Schema ** | | | | | | | | | | X |
| | | | | | | | | | | | |
| 101.CAL | | XBRL Taxonomy Definition ** | | | | | | | | | | X |
| | | | | | | | | | | | |
| 101.DEF | | XBRL Taxonomy Calculation ** | | | | | | | | | | X |
| | | | | | | | | | | | |
| 101.LAB | | XBRL Taxonomy Labels ** | | | | | | | | | | X |
| | | | | | | | | | | | |
| 101.PRE | | XBRL Taxonomy Presentation ** | | | | | | | | | | X |
| | | | | | | | | | | | |
| 104 | | Cover Page Interactive Data File (formatted in Inline XBRL and contained in Exhibit 101) | | | | | | | | | | X |
+ Previously filed
* The certifications furnished in Exhibit 32.1 and Exhibit 32.2 hereto are deemed to accompany this Annual Report on Form 10-K and will not be deemed “filed” for purposes of Section 18 of the Securities Exchange Act of 1934, as amended, except to the extent that the registrant specifically incorporates it by reference.
** The financial information contained in these XBRL documents is unaudited.
§ Indicates a management contract or compensatory plan or arrangement.
ITEM 16. FORM 10-K SUMMARY
None.
SIGNATURES
Pursuant to the requirements of Section 13 or 15(d) of the Securities Exchange Act of 1934, as amended, the Registrant has duly caused this Report to be signed on its behalf by the undersigned, thereunto duly authorized.
| | | | | | | | | | | |
| | Privia Health Group, Inc. |
| | | |
| Date: | February 27, 2026 | By: | /s/ Parth Mehrotra |
| | | Name: Parth Mehrotra |
| | | Title: Chief Executive Officer |
| | | |
Pursuant to the requirements of the Securities Exchange Act of 1934, this report has been signed below by the following persons on behalf of the registrant and in the capacities and on the dates indicated.
| | | | | | | | | | | | | | |
| Signature | | Title | | Date |
| | | | |
| /s/ Parth Mehrotra | | Chief Executive Officer and Director (principal executive officer) | | February 27, 2026 |
| Parth Mehrotra | | |
| | | | |
| /s/ David Mountcastle | | Executive Vice President and Chief Financial Officer (principal financial and accounting officer) | | February 27, 2026 |
| David Mountcastle | | |
| | | | |
/s/ Lance Berberian | | Director | | February 26, 2026 |
Lance Berberian | | |
| | | | |
| /s/ Nancy Cocozza | | Director | | February 27, 2026 |
| Nancy Cocozza | | |
| | | | |
| /s/ Pamela Kimmet | | Director | | February 27, 2026 |
| Pamela Kimmet | | |
| | | | |
| | | | |
| /s/ David King | | Director | | February 27, 2026 |
| David King | | |
| | | | |
| /s/ Thomas McCarthy | | Director | | February 27, 2026 |
| Thomas McCarthy | | |
| | | | |
| /s/ Shawn Morris | | Director | | February 27, 2026 |
| Shawn Morris | | |
| | | | |
| /s/ Jaewon Ryu | | Director | | February 27, 2026 |
| Jaewon Ryu, M.D. | | |
| | | | |
| /s/ David Wichmann | | Director | | February 27, 2026 |
| David Wichmann | | |
INDEX TO CONSOLIDATED FINANCIAL STATEMENTS
Report of Independent Registered Public Accounting Firm
To the Board of Directors and Stockholders of Privia Health Group, Inc.
Opinions on the Financial Statements and Internal Control over Financial Reporting
We have audited the accompanying consolidated balance sheets of Privia Health Group, Inc. and its subsidiaries (the "Company") as of December 31, 2025 and 2024, and the related consolidated statements of operations, of stockholders’ equity and of cash flows for each of the three years in the period ended December 31, 2025, including the related notes (collectively referred to as the "consolidated financial statements"). We also have audited the Company's internal control over financial reporting as of December 31, 2025, based on criteria established in Internal Control - Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO).
In our opinion, the consolidated financial statements referred to above present fairly, in all material respects, the financial position of the Company as of December 31, 2025 and 2024, and the results of its operations and its cash flows for each of the three years in the period ended December 31, 2025 in conformity with accounting principles generally accepted in the United States of America. Also in our opinion, the Company maintained, in all material respects, effective internal control over financial reporting as of December 31, 2025, based on criteria established in Internal Control - Integrated Framework (2013) issued by the COSO.
Basis for Opinions
The Company's management is responsible for these consolidated financial statements, for maintaining effective internal control over financial reporting, and for its assessment of the effectiveness of internal control over financial reporting, included in Management’s Annual Report on Internal Control over Financial Reporting appearing under Item 9A. Our responsibility is to express opinions on the Company’s consolidated financial statements and on the Company's internal control over financial reporting based on our audits. We are a public accounting firm registered with the Public Company Accounting Oversight Board (United States) (PCAOB) and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audits to obtain reasonable assurance about whether the consolidated financial statements are free of material misstatement, whether due to error or fraud, and whether effective internal control over financial reporting was maintained in all material respects.
Our audits of the consolidated financial statements included performing procedures to assess the risks of material misstatement of the consolidated financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the consolidated financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the consolidated financial statements. Our audit of internal control over financial reporting included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, and testing and evaluating the design and operating effectiveness of internal control based on the assessed risk. Our audits also included performing such other procedures as we considered necessary in the circumstances. We believe that our audits provide a reasonable basis for our opinions.
Definition and Limitations of Internal Control over Financial Reporting
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (i) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (ii) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (iii) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
Critical Audit Matters
The critical audit matters communicated below are matters arising from the current period audit of the consolidated financial statements that were communicated or required to be communicated to the audit committee and that (i) relate to accounts or disclosures that are material to the consolidated financial statements and (ii) involved our especially challenging, subjective, or complex judgments. The communication of critical audit matters does not alter in any way our opinion on the consolidated financial
statements, taken as a whole, and we are not, by communicating the critical audit matters below, providing separate opinions on the critical audit matters or on the accounts or disclosures to which they relate.
Valuation of Fee for Service Patient Care Accounts Receivable
As described in Notes 1 and 2 to the consolidated financial statements, substantially all of the Company’s accounts receivable arise from the provision of health care services to patients, the costs of which are primarily paid by federal and state governmental authorities or commercial insurance companies. The fee for service patient care (FFS-patient care) accounts receivable makes up a portion of the Company’s consolidated net accounts receivable balance of $400.9 million as of December 31, 2025. FFS-patient care revenue is primarily generated from third-party payers with which the Company has established contractual billing arrangements and is reported net of contractual allowances from third-party payers and patients. Management reports accounts receivable at the amount of consideration the Company expects to receive in exchange for providing healthcare services to patients, which is estimated using historical reimbursement rates and management’s analysis of prior collection experience, including expected contractual and other adjustments.
The principal considerations for our determination that performing procedures relating to the valuation of FFS-patient care accounts receivable is a critical audit matter are (i) the significant judgment by management when developing the estimated value of FFS-patient care accounts receivable; and (ii) a high degree of auditor judgment, subjectivity, and effort in performing procedures and evaluating audit evidence related to adjustments based on historical reimbursement rates.
Addressing the matter involved performing procedures and evaluating audit evidence in connection with forming our overall opinion on the consolidated financial statements. These procedures included testing the effectiveness of controls relating to management’s valuation of FFS-patient care accounts receivable. These procedures also included, among others, (i) evaluating management’s process for developing the estimated value of FFS-patient care accounts receivable, (ii) testing the completeness and accuracy of the underlying billing and reimbursement data used by management, (iii) evaluating the historical accuracy of management’s process for developing the estimated value of FFS-patient care accounts receivable, and (iv) developing an independent expectation of the estimated amount of FFS-patient care accounts receivable expected to be collected by management. Developing an independent expectation involved calculating historical reimbursement rates as compared to the recorded patient accounts receivable for historical periods and comparing that percentage to management’s estimated reimbursement rates used to determine the current year estimate for FFS-patient care accounts receivable.
Valuation of Medicare Shared Savings Program Revenue
As described in Notes 1 and 2 to the consolidated financial statements, under shared savings arrangements, the Company may earn financial incentives for increasing accountability over the cost, quality and efficiency of the care provided to the population of attributed members. Revenue from the Medicare Shared Savings Program (MSSP) makes up the majority of the Company’s consolidated shared savings revenue of $234.8 million for the year ended December 31, 2025. Incentive payments are earned when, for a given twelve-month measurement period, the Company meets or exceeds quality and utilization standards established by the payer and achieves savings on medical costs for the population of attributed members. To determine the amount of shared savings payments, payers evaluate the Company’s performance during the measurement period using the agreed-upon benchmarks, metrics and performance criteria. The Company estimates the transaction price by analyzing performance during the relevant time period in connection with the contractually defined benchmarks, metrics, performance criteria, inflation trends, risk adjustment factors, attribution criteria and other factors. Revenue is recognized only when the price can be reasonably estimated and it is probable that a significant reversal will not occur once any uncertainty associated with the variable consideration is subsequently resolved. Shared savings revenue is recorded in the period under which the underlying services are provided during the pre-set twelve-month measurement period.
The principal considerations for our determination that performing procedures relating to the valuation of MSSP revenue is a critical audit matter are (i) the significant judgment by management when developing the estimate of MSSP revenue; (ii) a high degree of auditor judgment , subjectivity , and effort in performing procedures and evaluating management’s significant assumptions related to inflation trend factors and risk ratio adjustments; and (iii) the audit effort involved the use of professionals with specialized skill and knowledge.
Addressing the matter involved performing procedures and evaluating audit evidence in connection with forming our overall opinion on the consolidated financial statements. These procedures included testing the effectiveness of controls relating to management’s valuation of MSSP revenue. These procedures also included, among others, (i) testing the completeness and accuracy of the underlying data used by management, and (ii) the involvement of professionals with specialized skill and knowledge to assist in evaluating the reasonableness of management’s estimate of MSSP revenue, on a sample basis, by (a) developing an independent range of estimated MSSP revenue using independently developed assumptions related to inflation trend factors and risk ratio adjustments and (b) comparing the independent range of estimated MSSP revenue to management’s estimate.
/s/ PricewaterhouseCoopers LLP
Washington, District of Columbia
February 27, 2026
We have served as the Company’s auditor since 2020, which includes periods before the Company became subject to SEC reporting requirements.
Privia Health Group, Inc.
Consolidated Balance Sheets
(in thousands, except share and per share amounts)
| | | | | | | | | | | |
| December 31, 2025 | | December 31, 2024 |
| Assets | | | |
| Current assets: | | | |
| Cash and cash equivalents | $ | 479,685 | | | $ | 491,149 | |
Accounts receivable, net of allowance for credit losses of $15.4 million and $9.3 million | 400,902 | | | 316,179 | |
| Prepaid expenses and other current assets | 30,414 | | | 27,495 | |
| Total current assets | 911,001 | | | 834,823 | |
| Non-current assets: | | | |
| Property and equipment, net | 504 | | | 1,242 | |
Right-of-use assets | 8,794 | | | 4,828 | |
| | | |
| Intangible assets, net | 215,919 | | | 109,807 | |
| Goodwill | 209,842 | | | 141,615 | |
Deferred tax asset, net | 2,274 | | | 26,383 | |
| Other non-current assets | 21,044 | | | 17,085 | |
| Total non-current assets | 458,377 | | | 300,960 | |
| Total assets | $ | 1,369,378 | | | $ | 1,135,783 | |
| | | |
| Liabilities and stockholders’ equity | | | |
| Current liabilities: | | | |
| Accounts payable and accrued expenses | $ | 96,804 | | | $ | 81,986 | |
| Provider liability | 469,516 | | | 364,607 | |
| | | |
| | | |
| Operating lease liabilities, current | 2,200 | | | 2,553 | |
| | | |
| Total current liabilities | 568,520 | | | 449,146 | |
| Non-current liabilities: | | | |
| | | |
| | | |
| | | |
| Operating lease liabilities, non-current | 7,331 | | | 3,037 | |
| Other non-current liabilities | 2,584 | | | 153 | |
| Total non-current liabilities | 9,915 | | | 3,190 | |
| Total liabilities | 578,435 | | | 452,336 | |
Commitments and contingencies (Note 13.) | | | |
| Stockholders’ equity: | | | |
Common stock, $0.01 par value, 1,000,000,000 shares authorized; 123,604,576 and 120,309,346 shares issued and outstanding at December 31, 2025 and December 31, 2024, respectively | 1,236 | | | 1,203 | |
| Additional paid-in capital | 892,291 | | | 813,209 | |
| Accumulated deficit | (156,310) | | | (179,229) | |
| Total Privia Health Group, Inc. stockholders’ equity | 737,217 | | | 635,183 | |
| Non-controlling interest | 53,726 | | | 48,264 | |
| Total stockholders’ equity | 790,943 | | | 683,447 | |
| Total liabilities and stockholders’ equity | $ | 1,369,378 | | | $ | 1,135,783 | |
The accompanying notes are an integral part of these consolidated financial statements.
Privia Health Group, Inc.
Consolidated Statements of Operations
(in thousands, except share and per share data)
| | | | | | | | | | | | | | | | | |
| For the Years Ended December 31, |
| 2025 | | 2024 | | 2023 |
| | | | | |
| Revenue | $ | 2,122,842 | | | $ | 1,736,390 | | | $ | 1,657,737 | |
| | | | | |
| Operating expenses: | | | | | |
| Provider expense | 1,660,680 | | | 1,332,537 | | | 1,298,573 | |
| Cost of platform | 252,732 | | | 227,000 | | | 197,663 | |
| Sales and marketing | 27,136 | | | 26,446 | | | 24,732 | |
| General and administrative | 138,152 | | | 126,157 | | | 109,587 | |
| Depreciation and amortization | 9,907 | | | 7,268 | | | 6,533 | |
| Total operating expenses | 2,088,607 | | | 1,719,408 | | | 1,637,088 | |
Operating income | 34,235 | | | 16,982 | | | 20,649 | |
Interest income, net | 9,703 | | | 10,888 | | | 8,372 | |
Income before provision for income taxes | 43,938 | | | 27,870 | | | 29,021 | |
Provision for income taxes | 14,212 | | | 10,826 | | | 7,993 | |
Net income | 29,726 | | | 17,044 | | | 21,028 | |
| Less: Net income (loss) attributable to non-controlling interests | 6,807 | | | 2,659 | | | (2,051) | |
Net income attributable to Privia Health Group, Inc. | $ | 22,919 | | | $ | 14,385 | | | $ | 23,079 | |
Net income per share attributable to Privia Health Group, Inc. stockholders – basic | $ | 0.19 | | | $ | 0.12 | | | $ | 0.20 | |
Net income per share attributable to Privia Health Group, Inc. stockholders – diluted | $ | 0.18 | | | $ | 0.11 | | | $ | 0.19 | |
| Weighted average common shares outstanding – basic | 122,176,587 | | | 119,402,749 | | | 116,731,406 | |
| Weighted average common shares outstanding – diluted | 128,889,836 | | | 125,614,171 | | | 124,686,067 | |
The accompanying notes are an integral part of these consolidated financial statements.
Privia Health Group, Inc.
Consolidated Statements of Stockholders’ Equity
(in thousands except share amounts)
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | Common Stock Shares | | Common Stock | | Additional Paid-in Capital | | Accumulated Deficit | | Total Stockholders’ Equity attributable to Privia Health Group, Inc. | | Non-controlling Interest | | Total Stockholders’ Equity |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
| | | | | | | | | | | | | | |
| Balance at January 1, 2023 | | 114,690,808 | | | 1,148 | | | 714,639 | | | (216,693) | | | 499,094 | | | 19,955 | | | 519,049 | |
| Common stock issued | | 3,526,171 | | | 34 | | | 8,706 | | | — | | | 8,740 | | | — | | | 8,740 | |
| Stock-based compensation expense | | — | | | — | | | 37,098 | | | — | | | 37,098 | | | — | | | 37,098 | |
| Repurchase of non-controlling interest | | — | | | — | | | (8,871) | | | — | | | (8,871) | | | 3,177 | | | (5,694) | |
| Contributed non-controlling interest | | — | | | — | | | — | | | — | | | — | | | 24,871 | | | 24,871 | |
| Tax effect related to purchase of non-controlling interest | | — | | | — | | | 2,297 | | | — | | | 2,297 | | | — | | | 2,297 | |
| Net income (loss) | | — | | | — | | | — | | | 23,079 | | | 23,079 | | | (2,051) | | | 21,028 | |
| Balance at December 31, 2023 | | 118,216,979 | | | 1,182 | | | 753,869 | | | (193,614) | | | 561,437 | | | 45,952 | | | 607,389 | |
| Common stock issued | | 2,092,367 | | | 21 | | | 2,660 | | | — | | | 2,681 | | | — | | | 2,681 | |
| Stock-based compensation expense | | — | | | — | | | 56,680 | | | — | | | 56,680 | | | — | | | 56,680 | |
| Contributed non-controlling interest | | — | | | — | | | — | | | — | | | — | | | 1,653 | | | 1,653 | |
| Distribution to non-controlling interest | | — | | | — | | | — | | | — | | | — | | | (2,000) | | | (2,000) | |
| Net income | | — | | | — | | | — | | | 14,385 | | | 14,385 | | | 2,659 | | | 17,044 | |
| Balance at December 31, 2024 | | 120,309,346 | | | 1,203 | | | 813,209 | | | (179,229) | | | 635,183 | | | 48,264 | | | 683,447 | |
| Common stock issued | | 3,295,230 | | | 33 | | | 8,014 | | | — | | | 8,047 | | | — | | | 8,047 | |
| Stock-based compensation expense | | — | | | — | | | 71,068 | | | — | | | 71,068 | | | — | | | 71,068 | |
| | | | | | | | | | | | | | |
| Distribution to non-controlling interest | | — | | | — | | | — | | | — | | | — | | | (1,345) | | | (1,345) | |
| Net income | | — | | | — | | | — | | | 22,919 | | | 22,919 | | | 6,807 | | | 29,726 | |
| Balance at December 31, 2025 | | 123,604,576 | | | $ | 1,236 | | | $ | 892,291 | | | $ | (156,310) | | | $ | 737,217 | | | $ | 53,726 | | | $ | 790,943 | |
The accompanying notes are an integral part of these consolidated financial statements.
Privia Health Group, Inc.
Consolidated Statements of Cash Flows
(in thousands)
| | | | | | | | | | | | | | | | | |
| For the Years Ended December 31, |
| 2025 | | 2024 | | 2023 |
| Cash flows from operating activities | | | | | |
Net income | $ | 29,726 | | | $ | 17,044 | | | $ | 21,028 | |
Adjustments to reconcile net income to net cash provided by operating activities: | | | | | |
| Depreciation | 739 | | | 1,104 | | | 1,174 | |
| Amortization of intangibles | 9,168 | | | 6,164 | | | 5,359 | |
| Stock-based compensation | 71,068 | | | 56,680 | | | 37,098 | |
Deferred income taxes | 10,871 | | | 8,817 | | | 7,465 | |
| Changes in asset and liabilities: | | | | | |
Accounts receivable, net | (36,668) | | | (19,824) | | | (96,877) | |
| Prepaid expenses and other current assets | (1,599) | | | (8,970) | | | (6,159) | |
Other non-current assets and right-of-use assets | (326) | | | (1,721) | | | (2,418) | |
| Accounts payable and accrued expenses | 14,824 | | | 19,905 | | | 4,994 | |
| Provider liability | 65,629 | | | 32,942 | | | 113,367 | |
| Operating lease liabilities | (2,459) | | | (2,699) | | | (3,214) | |
| Other long-term liabilities | 2,431 | | | (160) | | | (1,032) | |
| Net cash provided by operating activities | 163,404 | | | 109,282 | | | 80,785 | |
| Cash flows from investing activities | | | | | |
Acquisitions, net of cash acquired | (180,370) | | | (6,957) | | | (42,858) | |
Other | (1,200) | | | (5,021) | | | (113) | |
| Net cash used in investing activities | (181,570) | | | (11,978) | | | (42,971) | |
| Cash flows from financing activities | | | | | |
Repurchase of non-controlling interest | — | | | — | | | (5,694) | |
| Proceeds from non-controlling interest | — | | | 1,653 | | | 659 | |
Distribution to non-controlling interest | (1,345) | | | — | | | — | |
| Proceeds from exercised stock options | 8,047 | | | 2,681 | | | 8,740 | |
Net cash provided by financing activities | 6,702 | | | 4,334 | | | 3,705 | |
Net (decrease) increase in cash and cash equivalents | (11,464) | | | 101,638 | | | 41,519 | |
| Cash and cash equivalents at beginning of period | 491,149 | | | 389,511 | | | 347,992 | |
| Cash and cash equivalents at end of period | $ | 479,685 | | | $ | 491,149 | | | $ | 389,511 | |
| | | | | |
| Supplemental disclosure of cash flow information: | | | | | |
| Interest paid | $ | 251 | | | $ | 285 | | | $ | 40 | |
Income taxes paid, net of refunds | $ | 6,639 | | | $ | 3,755 | | | $ | 1,040 | |
| | | | | |
Supplemental disclosure of non-cash operating activities: | | | | | |
Leases liabilities obtained in exchange for right-of-use assets | $ | 6,400 | | | $ | — | | | $ | — | |
| | | | | |
The accompanying notes are an integral part of these consolidated financial statements.
Privia Health Group, Inc.
Notes to Consolidated Financial Statements
1.Organization and Summary of Significant Accounting Policies
Organization
Privia Health Group, Inc. (“Privia Health”, “Privia”, “we”, “our” or the “Company”) is a technology-driven, national physician-enablement company that collaborates with physician practices, health plans, and health systems to achieve the quadruple aim of better outcomes, lower costs, improved patient experience, and greater provider engagement and satisfaction. The Company pursues the quadruple aim by entering markets and organizing existing physicians and non-physician clinicians into a unique practice model that combines the advantages of a partnership in a large regional medical group (each, a “Medical Group”) with significant provider autonomy for physicians (collectively, “Privia Physicians”) and non-physician clinicians (collectively, “Privia Clinicians” and, together with the Privia Physicians, the “Privia Providers”) joining the Company’s Medical Groups.
As of December 31, 2025, Privia operated in sixteen markets: 1) the Mid-Atlantic Region (states of Virginia, Maryland and the District of Columbia); 2) Georgia; 3) Gulf Coast Region (Houston-San Antonio-Austin, Texas); 4) North Texas (Dallas/Fort Worth, Texas); 5) West Texas (Abilene, Texas); 6) Florida; 7) Tennessee 8) California; 9) Montana; 10) Ohio; 11) North Carolina; 12) Connecticut; 13) Washington state; 14) South Carolina; 15) Indiana; and 16) Arizona.
Under our Privia Medical Group model, Privia Physicians join the Medical Group in their geographic market as an owner of the Medical Group. We own a majority interest in certain of our Medical Groups (each, an “Owned Medical Group”), with Privia Physicians collectively owning a minority interest, and we own no interest in certain other Medical Groups for which we provide services through a management agreement (each, a “Non-Owned Medical Group”). In those markets in which state regulations prohibit us from owning Medical Groups, the Non-Owned Medical Groups may be owned by the Privia Physicians or owned indirectly through a professional entity (a “Nominee PC”) by a licensed physician holding a Privia leadership position (such physician leader, a “Nominee Physician”, and each such Non-Owned Medical Group owned in this manner, a “Friendly Medical Group”). In those markets where we partner with health systems, our health system partner owns a majority interest in the Non-Owned Medical Groups, with Privia Physicians owning a minority interest. Privia Physicians furnish healthcare services through our Medical Groups and continue to own their historical practice entities (“Affiliated Practices”), which provide certain services to the Medical Groups, such as use of space, non-physician staffing, equipment and supplies. Privia Physicians typically enter into a physician member services agreement (“PMSA”) with a medical group, which requires the Privia Physician to provide healthcare services through and on behalf of the medical group, and the Medical Group enters into a Support Services Agreement (“SSA”) with the Affiliated Practice to provide those certain services to the Medical Group.
In some instances, we also move into and expand in new and existing markets through our Privia Care Partners model, which offers an affiliation model to providers who are looking solely for value-based care (“VBC”) solutions. For those practices, we furnish population health services, reporting and analytics, in addition to certain management services.
The Company does not own any Affiliated Practice, and does not bear risk of loss related to the Affiliated Practices which are typically owned by certain Privia Physicians. As of the reporting date, the Company has Friendly Medical Groups in Tennessee, West Texas, Washington state, South Carolina and Indiana. The Company has entered into a restriction agreement with each of its Nominee Physicians and their respective Nominee PCs, which grant the Company, among other rights, the ability to direct the transfer of each Nominee PC’s ownership rights in the Friendly Medical Groups to other licensed physicians. We consolidate Owned Medical Groups and Friendly Medical Groups into our financial statements, while we do not consolidate Non-Owned Medical Groups. For further information on Non-Owned Medical Groups and Friendly Medical Groups, please refer to “Variable Interest Entities”.
The Company also provides management services through local management services organizations (each, an “MSO”) to the Medical Groups through a Management Services Agreement (“MSA”) in each market. The Company owns 100% of all MSOs, except seven where the Company holds a majority ownership interest.
We derive our revenues from the following three principal sources: (i) FFS-patient care revenue from the provision of healthcare services to patients through Privia Providers of Owned Medical Groups and Friendly Medical Groups, in addition to management and administrative services earned for administrative services provided to Non-Owned Medical Groups (“FFS-administrative services”), (ii) VBC revenue collected on behalf of our Privia Providers in the form of (a) capitated revenue and (b) management and administrative fees, which primarily consist of shared savings, including quality bonuses, and per member per month (“PMPM”) care management fees, as well as (iii) other revenue from additional services offered to Privia Providers or directly to patients or employers, including ancillary services such as clinical lab, pharmacy and imaging services. The operations of our Owned Medical Groups, owned Accountable Care Organizations (“ACO”), owned MSOs and Friendly Medical Groups are reflected within our consolidated financial results.
Basis of Presentation
The consolidated financial statements are prepared in accordance with United States generally accepted accounting principles (“GAAP”) and include the accounts of the Company and its subsidiaries. Amounts shown on the consolidated statements of operations
within the operating expense categories of provider expense, cost of platform, selling and marketing, and general and administrative are recorded exclusive of depreciation and amortization.
All significant intercompany transactions are eliminated in consolidation.
Variable Interest Entities
Management evaluates the Company’s ownership, contractual, and other interests to determine if the Company holds a variable interest in a variable interest entity (“VIE”). These evaluations are complex, involve judgment, including the use of estimates and assumptions based on available historical information, among other factors. If the Company determines that an entity in which it holds a contractual or ownership interest is a VIE and that the Company is the primary beneficiary, the Company consolidates such entity in its consolidated financial statements. The primary beneficiary of a VIE is the party that meets both of the following criteria: (i) has the power to make decisions that most significantly affect the economic performance of the VIE; and (ii) has the obligation to absorb losses or the right to receive benefits that in either case could potentially be significant to the VIE. Management periodically reassesses whether changes in the facts and circumstances regarding the Company’s involvement with a VIE, or other arrangements, result in a change to the consolidation conclusion. Any such changes in consolidation status are applied prospectively.
The Company evaluates its relationship with (a) Non-Owned Medical Groups and their Affiliated Practices, (b) Friendly Medical Groups and their Affiliated Practices, (c) Affiliated Practices associated with Owned Medical Groups and (d) Owned Medical Groups it forms or acquires, to determine if any of these entities should be consolidated into the Company’s financial statements. The Company does not have an ownership interest in any Affiliated Practices (whether those of Owned Medical Groups, Non-Owned Medical Groups or Friendly Medical Groups); nor does the Company have an ownership interest in Non-Owned Medical Groups or Friendly Medical Groups. The PMSA and SSA entered into by Non-Owned Medical Groups and Friendly Medical Groups with their Privia Physician members and the Affiliated Practices are not contractual relationships within Privia’s legal structure. The only contractual relationship between Privia and Non-Owned Medical Groups is established through the MSA. For Friendly Medical Groups, in addition to the MSA, the Company has a contractual relationship, evidenced by a restriction agreement (each a “Restriction Agreement”) with its Nominee Physicians and their respective Nominee PCs. Management has determined, based on the provisions of the MSAs between the Company and Non-Owned Medical Groups, and after considering the requirements of Accounting Standards Codification (“ASC”) Topic 810, Consolidation (“ASC 810”), that the Company is not required to consolidate the financial position or results of operations of (i) Affiliated Practices associated with Owned Medical Groups; (ii) Non-Owned Medical Groups or, (iii) Affiliated Practices of a Non-Owned Medical Group. However, management has determined, based on the provisions of the Restriction Agreement by and among the Company, the Nominee Physicians and their respective Nominee PCs, the governing documents of the Friendly Medical Groups, and after considering the requirements of ASC 810, that the Company should consolidate the financial position and results of operations of the Friendly Medical Groups and the Nominee PCs, but not the Affiliated Practices of the Friendly Medical Groups.
ASC 810 requires the Company to consolidate the financial position, results of operations and cash flows of a Non-Owned Medical Group affiliated by means of a service agreement if the Non-Owned Medical Group is a VIE and the Company is its primary beneficiary. A Non-Owned Medical Group would be considered a VIE if (a) it is thinly capitalized (i.e., the equity is not sufficient to fund the Non-Owned Medical Group’s activities without additional subordinated financial support) or (b) the equity holders of the Non-Owned Medical Group as a group have one of the following four characteristics: (i) lack the power to direct the activities that most significantly affect the Non-Owned Medical Group’s economic performance, (ii) possess non-substantive voting rights, (iii) lack the obligation to absorb the Non-Owned Medical Group’s expected losses, or (iv) lack the right to receive the Non-Owned Medical Group’s expected residual returns.
The characteristics of both (a) and (b) do not exist and as such the Non-Owned Medical Groups do not represent VIEs. Accordingly, the Company has not consolidated the financial position, results of operations or cash flows of the Non-Owned Medical Groups that are affiliated with the Company by means of a service agreement for the years ended December 31, 2025, 2024, and 2023. Each time the Company enters into a new service agreement, or enters into a material amendment to an existing service agreement, with a Medical Group, the Company considers whether the terms of that agreement or amendment would change the elements it considers in accordance with the VIE guidance. Management performed this analysis for Affiliated Practices of Owned Medical Groups, which have contractual relationships with Privia through the SSA, and determined these entities do not represent VIEs pursuant to ASC 810 criteria and therefore are not consolidated.
The Company, however, does meet the criteria for consolidation of the Owned Medical Groups, Nominee PCs and the Friendly Medical Groups based on ASC 810 criteria.
Privia Medical Group – West Texas, PLLC, (“PMG West Texas”) is a physician-owned Medical Group, with PMG West Texas Holdings, PLLC (“Friendly WTX PC”), a Texas professional limited liability company wholly owned by a Nominee Physician, owning majority membership interests and having governance and control rights via the governing documents of PMG West Texas. The Company has a contractual relationship with Friendly WTX PC through a Restriction Agreement. The VIE analysis was performed, and the Company determined that characteristic (b) exists as a result of meeting (i), (ii) and (iv) and, as such, PMG West Texas and Friendly WTX PC do represent VIEs and are consolidated as they do meet the criteria in ASC 810.
Privia Medical Group Tennessee, PLLC (“PMG-TN”) is a physician-owned Medical Group, with PMG-TN Physicians, PLLC (“Friendly TN PC”), a Tennessee professional limited liability company wholly owned by a Nominee Physician, owning majority membership interests therein and having governance and control rights via the governing documents of PMG-TN. Again, the same analysis was performed, and the Company determined that characteristic (b) exists as a result of meeting (i), (ii) and (iv) and, as such, PMG-TN and Friendly TN PC do represent VIEs as they do meet the criteria in ASC 810.
Privia Medical Group Washington, PLLC, (“PMG WA”) is a physician-owned Medical Group, with PMG Washington Holdings, PLLC (“Friendly WA PC”), a Washington professional limited liability company wholly owned by a Nominee Physician, owning majority membership interests and having governance and control rights via the governing documents of PMG WA. The Company has a contractual relationship with Friendly WA PC through a Restriction Agreement. The VIE analysis was performed, and the Company determined that characteristic (b) exists as a result of meeting (i), (ii) and (iv) and, as such, PMG WA and Friendly WA PC do represent VIEs and are consolidated as they do meet the criteria in ASC 810.
Privia Medical Group South Carolina, LLC, (“PMG SC”) is a physician-owned Medical Group, with PMG South Carolina Holdings, PLLC (“Friendly SC PC”), a South Carolina professional limited liability company wholly owned by a Nominee Physician, owning majority membership interests and having governance and control rights via the governing documents of PMG SC. The Company has a contractual relationship with Friendly SC PC through a Restriction Agreement. The VIE analysis was performed, and the Company determined that characteristic (b) exists as a result of meeting (i), (ii) and (iv) and, as such, PMG SC and Friendly SC PC represent VIEs and are consolidated as they meet the criteria in ASC 810.
Privia Medical Group Indiana, LLC, (“PMG IN”) is a physician-owned Medical Group, with PMG Holdings Indiana, LLC, (“Friendly IN PC”), an Indiana professional limited liability company wholly owned by a Nominee Physician, owning majority membership interests and having governance and control rights via the governing documents of PMG IN. The Company has a contractual relationship with Friendly IN PC through a Restriction Agreement. The VIE analysis was performed, and the Company determined that characteristic (b) exists as a result of meeting (i), (ii) and (iv) and, as such, PMG IN and Friendly IN PC represent VIEs and are consolidated as they meet the criteria in ASC 810.
Privia Medical Group Arizona, PLLC ("PMG-AZ") is an Owned Medical Group, with the Company owning a majority of the membership interests and having governance and control rights through the governing documents of PMG-AZ. The VIE analysis was performed, and the Company determined that characteristic (a) exists, and, as such, PMG-AZ does represent a VIE and is consolidated as it does meet the criteria in ASC 810.
The aggregated carrying value of the VIE assets and liabilities included in the consolidated balance sheets after elimination of intercompany transactions and balances each were $18.9 million and $12.1 million as of December 31, 2025 and 2024, respectively. Total revenues and operating expenses were each $215.5 million, $104.5 million, and $61.1 million for the years ended December 31, 2025, 2024, and 2023, respectively.
Use of Estimates
The preparation of consolidated financial statements in conformity with GAAP requires management to make estimates and assumptions that affect the reported amounts of assets, liabilities, revenue, expenses, and related disclosures. On an on-going basis, management evaluates its significant estimates and assumptions, including, but not limited to, revenue recognition, stock-based compensation, estimated useful lives of assets, intangible assets subject to amortization, the fair value of assets acquired and liabilities assumed in business combinations, and the provision for income taxes. These estimates are based on historical experience, current conditions, and other assumptions that management believes are reasonable under the circumstances. Actual results could differ from those estimates. Estimates and assumptions are reviewed and updated as new information becomes available, additional experience is gained, future events occur, or the Company’s operating environment changes.
Operating Segments
In accordance with ASC 280, Segment Reporting (“ASC 280”) the Company has determined that it operates in a single operating segment, and accordingly, reports one reportable segment – Privia Health Group, Inc. Refer to Note 16. “Segment Financial Information” for additional information regarding the Company’s services.
Cash and Cash Equivalents
The Company considers all unrestricted, liquid financial instruments purchased with original maturity dates of three months or less to be cash equivalents. Cash equivalents are stated at cost which approximates fair value.
Accounts Receivable
Substantially all of the Company’s accounts receivable arise from the provision of health care services to patients, the costs of which are primarily paid by federal and state governmental authorities or commercial insurance companies. Accounts receivable are recorded at the amount of consideration the Company expects to receive in exchange for providing healthcare services to patients, which is
estimated using historical reimbursement rates and management’s analysis of prior collection experience, including expected contractual and other adjustments.
Accounts receivable are written off when they are deemed uncollectible due to circumstances that affect the ability of third-party payers or self-pay patients to remit payments. While write-offs have historically been within management’s expectations and the related allowances established, future write-offs may differ from historical experience, and could result in material differences between actual results and the Company’s recorded allowances.
Unearned Revenue
The Company records unearned revenue, which is a contract liability, when payment is received prior to the Company’s obligated performance of the related services.
Property and Equipment, Net
Property and equipment consist of furniture and fixtures, leasehold improvements, and computer hardware and software. Property and equipment are stated at cost less accumulated depreciation and amortization. Depreciation is recognized using the straight-line method over the estimated useful lives of the related assets. The estimated useful life of leasehold improvements is the lesser of the lease term or useful life of the asset, while other property and equipment are depreciated over estimated useful lives, generally ranging from three to seven years.
Business Combinations
Accounting for business combinations requires the allocation of the fair value of the purchase consideration to the identifiable tangible and intangible assets acquired, and liabilities assumed based on their estimated fair values, which are determined primarily using income-based valuation methods. The excess of the fair value of the purchase consideration over the fair values of these identifiable net assets acquired is recorded as goodwill. These valuations require the use of significant estimates and assumptions, particularly with respect to intangible assets. Significant assumptions used in valuing intangible assets include, but are not limited to, projected revenue growth rates and attrition, medical claims expense, cost of care, operating expenses, discount rates, contract terms and the estimated useful lives of the acquired assets.
The Company’s estimates of fair value are based on assumptions management believes to be reasonable; however, such assumptions are inherently uncertain and unpredictable and, as a result, actual results may differ from those estimates. The allocation of purchase consideration to identifiable assets acquired and liabilities assumed affects the Company’s amortization expense, as acquired finite-lived intangible assets are amortized over their estimated useful lives. Indefinite-lived intangible assets, including goodwill, are not amortized. During the measurement period, which does not exceed one year from the acquisition date, the Company may record adjustments to the amounts initially recorded with a corresponding offset to goodwill. Upon conclusion of the measurement period, any subsequent adjustments are recognized in earnings.
During the years ended December 31, 2025, and 2024, the Company completed several acquisitions to strengthen its market position in existing markets and to expand into new markets. The consideration paid in each acquisition was determined through arm’s-length negotiations. Each acquisition was accounted for using the acquisition method pursuant to the requirements of Financial Accounting Standards Board (“FASB”) ASC Topic 805, Business Combinations (“ASC 805”). The results of operations of the acquisitions have been included in the Company’s consolidated financial statements since their respective acquisition date. For additional information, refer to Note 3. “Business Combinations.”
Impairment of Long-Lived Assets
Long-lived assets consist of property and equipment. Long-lived assets to be held and used are tested for recoverability whenever events or changes in business circumstances indicate that the carrying amount of the assets may not be fully recoverable. Factors considered in determining whether an impairment review is required include significant underperformance in relation to expectations, adverse industry or economic trends and significant changes or planned changes in the manner in which the assets are used. If an impairment review is performed, the Company assesses recoverability by comparing the carrying value of the long-lived asset group to the sum of the undiscounted future cash flows expected to result from the use and eventual disposition of the long-lived asset group. If the carrying amount exceeds the undiscounted future cash flows, an impairment loss is recognized. The impairment loss is based on the excess of the carrying value of the impaired asset group over its fair value, determined using discounted cash flows. The Company did not record any impairment losses on long-lived assets during the years ended December 31, 2025, 2024, or 2023.
Goodwill
Goodwill represents the excess of the purchase price, plus the fair value of any non-controlling interests in the acquiree, over the fair value of identifiable net assets acquired. The Company performs a qualitative assessment on goodwill at least annually or more frequently if events or changes in circumstances indicate that the carrying value of goodwill may not be recoverable. If the qualitative assessment indicates that the fair value of a reporting unit is more likely than not below its carrying amount, the Company performs a quantitative impairment test. The quantitative goodwill impairment test compares the fair value of the reporting unit with its carrying amount. Any excess of the carrying value over the fair value is recognized as an impairment loss, limited to the total amount of
goodwill allocated to that reporting unit. The Company has a single reporting unit and accordingly performs a single assessment of goodwill.
For the years ended December 31, 2025, 2024, and 2023, there was no impairment loss related to goodwill. For additional information, refer to Note 4. “Goodwill and Intangible Assets, Net.”
Intangible Assets, net
Definite-lived intangible assets represent the estimated fair value of identifiable intangible assets acquired. These assets are amortized using the straight-line method over their estimated useful lives as follows:
| | | | | |
| Trade names | 20 years |
| Consumer customer relationships | 10 - 24 years |
| |
Management Service Agreement | 16 years |
| Physician network | 10 - 15 years |
| Payer contracts | 10 - 22 years |
MSO Service Agreements | 21 years |
The Company evaluates its finite-lived intangible assets for impairment whenever events or changes in circumstances indicate that the carrying amount of an asset may not be recoverable. Recoverability is assessed by comparing the carrying amount of the asset to the sum of the undiscounted future cash flows expected to result from the use and eventual disposition of the asset. If the carrying amount exceeds the undiscounted future cash flows, the asset is written down to its fair value, which is determined based on estimated discounted future cash flows. In performing this assessment, management considers, among other factors, current operating results, forecast, the manner in which the intangible assets are used, and the effects of obsolescence, demand, competition, and other economic factors. Based on these assessments, no impairment loss was recorded for the years ended December 31, 2025, 2024, and 2023. For additional information, refer to Note 4. “Goodwill and Intangible Assets, Net.”
Debt Issuance Costs
Debt issuance costs represent costs incurred in connection with the issuance of debt. When debt is outstanding, these costs are recorded as a direct reduction of the related debt. When no debt is outstanding, debt issuance costs are recorded as an asset. Debt issuance costs are amortized over the term of the arrangement using the effective interest method and included in interest expense in the accompanying consolidated statements of operations.
Revenue Recognition
The Company derives revenues from the following three sources: (i) FFS revenue, (ii) VBC revenue and (iii) other revenue from additional services offered by Privia to its Privia Providers or directly to patients or employers. To determine revenue recognition for arrangements that are within the scope of Accounting Standards Codification (“ASC”) Topic 606, Revenue from Contracts with Customers (“ASC 606”), the Company applies the following five-step model:
i.Identify the contract(s) with a customer;
ii.Identify the performance obligations in the contract;
iii.Determine the transaction price;
iv.Allocate the transaction price to the performance obligations in the contract; and
v.Recognize revenue as the entity satisfies a performance obligation.
FFS Revenue
FFS-patient care
The Company’s FFS-patient care revenue is primarily generated from the provision of healthcare services to patients. The provision of medical services represents a single performance obligation under the Company’s third-party payer arrangements, and accordingly, the transaction price is allocated entirely to that performance obligation. Revenue is recognized as services are rendered and approved by Privia Providers, which typically occurs on the same day the services are provided. Payment for services are received from third-party payers and, in certain cases, from patients who are insured but are financially responsible for a portion of the services through co-payments, coinsurance, or deductibles. Patients without health insurance are generally required to pay for services in full.
FFS-patient care revenue is reported net of contractual allowances from third-party payers and patients. The Company has certain agreements with third-party payers that provide for reimbursement at amounts different from the Company’s standard billing rates. The differences between the estimated reimbursement rates and the standard billing rates are recorded as contractual adjustments, and are deducted from gross revenue to arrive at FFS-patient care revenue. The Company estimates implicit price concessions based on historical collection experience by patient class using a portfolio approach as a practical expedient rather than estimating individually.
The financial statement effects of applying this practical expedient are not materially different from those that would result from an individual contract approach. Subsequent changes in estimates of the transaction price including those determined on a portfolio basis when applicable are generally recorded as adjustments to revenue in the period in which the change occurs. For the years ended December 31, 2025, 2024, and 2023, changes in the Company’s estimates of implicit price concessions, contractual adjustments, and expected payments for performance obligations satisfied in prior periods were not significant.
With respect to fee-for-service (“FFS”) patient care revenue generated by Owned Medical Groups and Friendly Medical Groups, the Company evaluated whether it acts as a principal or an agent under ASC 606, given that healthcare services are furnished by Privia Providers rather than employees of the Medical Groups. ASC 606-10-55-37A states that an entity is a principal if it obtains control of a right to a service to be performed by another party, which provides the entity with the ability to direct that party to perform the service on the entity’s behalf. The Owned Medical Groups, which are majority-owned and controlled by the Company, own the contractual relationships with the patients and the third-party payers, and they direct Privia Providers to perform healthcare services on the Company’s behalf. Although the Company is prohibited by law from interfering in the physician-patient relationship or making clinical care decisions, the Company’s Owned Medical Groups are responsible for the fulfillment of healthcare services to patients. Further, the Company employs Chief Medical Officers and Medical Directors who provide clinical oversight and direction over the clinical affairs of the Owned Medical Groups. Owned Medical Groups provide the care coordination activities, patient outreach and education activities, and set quality standards for Privia Providers. The Company verifies that Privia Providers have the proper qualifications (e.g., correct licenses, certificates, etc.) for the Company’s Owned Medical Groups, for the Company and as a delegate on behalf of certain third-party payers. In addition to overseeing health care services, Owned Medical Groups are primarily responsible for delivering services to patients and retain discretion in establishing pricing through agreements with patients and their insurance payers. The Owned Medical Groups also negotiate and enter into provider agreements with third-party payer insurance companies, which define the respective obligations of Owned Medical Groups and the third-party payers including reimbursement rates for all services provided.
In assessing who is the principal in providing the patient care services, the Company considered who controls the provision of patient care services. Based on the Company’s oversight of Owned Medical Groups (including setting the expectations for the Owned Medical Group’s patients and the commercial payers’ expectations of the Owned Medical Groups) and the contractual relationships with patients and their third-party payers, the Company concluded it is the principal in these arrangements.
FFS-administrative services
The Company’s FFS-administrative services business provides administration and management services pursuant to MSAs with Non-Owned Medical Groups. The MSAs with the Non-Owned Medical Groups range from 5 – 20 years in duration and outline the terms and conditions of the administration and management services to be provided, including revenue cycle management services such as billings and collections, as well as other services, including, but not limited to, payer contracting, information technology services, accounting and treasury services.
Under certain MSAs, the Company is compensated for administrative services equal to the cost of providing specified services, including a fixed margin, if applicable. While the margin is fixed, the cost of providing services may fluctuate over the life of the contract. In other MSAs, the Company is paid a fixed percentage of net collections though the net collections may vary over time.
Each MSA constitutes a single performance obligation to provide a series of administration and management services over the contract period. The Company has determined that each Non-Owned Medical Group receives the services daily and has concluded that an output method is appropriate for recognizing administrative services fee revenue.
Administrative fee revenue is reported at the amount that reflects the consideration to which the Company expects to be entitled in exchange for the provision of administration and management services to the Non-Owned Medical Groups. Certain MSAs include provisions for rebates to customers if specified conditions are met. The Company estimates the transaction price for such variable consideration using the most likely amount method and includes these amounts in the net transaction price to the extent that it is probable that a significant reversal will not occur when the uncertainty is resolved. FFS-administrative services revenue is reduced by the amount of any rebates earned by customers. Rebates of $3.5 million, $1.8 million, and $2.7 million were recorded for the years ended December 31, 2025, 2024, and 2023, respectively.
VBC Revenue
The Company’s VBC business consists of its clinically integrated networks and ACOs which bring together independent physician practices within the Company medical groups to share data, improve care coordination, and collaborate on initiatives designed to improve outcomes and reduce healthcare spending. The Company has multi-year contracts with the U.S. federal government and large payer organizations typically ranging from three to five years. Payments under these contracts are made in the following forms: (1) capitated revenue, (2) shared savings, and (3) care management fees on a per member per month basis.
Capitated Revenue
Capitated revenue represents fees earned under contracts with various Medicare Advantage payers (“Payers”) in at-risk capitation arrangements. Under these arrangements, the Company is entitled to monthly fees for the provision of a defined range of healthcare
services for Medicare Advantage health plan members (“attributed beneficiaries” or “attributed lives”) assigned to the Company’s contracted physicians, typically primary care providers. Monthly fees are calculated as a percentage of the premium Payers receive from the Centers for Medicare & Medicaid Services (“CMS”) for these attributed beneficiaries. In at-risk arrangements, the Company generally accepts financial risk for beneficiaries attributed to its contracted physicians and, is responsible for the cost of contracted healthcare services required by those beneficiaries in accordance with the terms of the agreement. Fees are recorded gross in revenue because the Company is acting as a principal in coordinating and controlling the range of services provided (other than clinical decisions) under its capitation contracts. Capitated contracts are generally multi-year arrangements and contain a single performance obligation representing the stand-ready obligation to provide all necessary medical care to members over the contract period. Revenue is recognized in the month during which each eligible beneficiary is entitled to receive healthcare benefits.
The capitation contract transaction price is a fixed percentage of premium per attributed life subject to periodic adjustment under CMS’s risk adjustment payment methodology. CMS determines premiums based on each attributed life’s health status and certain demographic factors, using diagnosis data submitted by both the Company and healthcare providers. The Company estimates adjustments to capitated revenue using the most likely amount methodology and includes in revenue only to the extent that it is probable that a significant reversal of cumulative revenue will not occur once any uncertainty is resolved. Capitated revenue is also subject to adjustments for incentives or penalties tied to the achievement of quality metrics defined in the Company’s contracts. Incentive revenue is recognized using the most likely amount methodology and only to the extent that it is probable that a significant reversal of cumulative revenue will not occur once the uncertainty is resolved.
Neither the Company nor any of its affiliates are a registered insurance company, as state law in the states in which the Company operates do not require such registration for risk bearing providers.
Shared Savings
Under shared savings arrangements, the Company may earn financial incentives for increasing accountability over the cost, quality and efficiency of the care provided to attributed members. Incentive payments are earned when, for a given twelve-month measurement period, the Company meets or exceeds quality and utilization standards established by the payer and achieves savings on medical costs for the population of attributed members. To determine the amount of shared savings payments, payers evaluate the Company’s performance during the measurement period using agreed-upon benchmarks, metrics and performance criteria.
The Company estimates the transaction price by analyzing performance during the relevant time period in connection with the contractually defined benchmarks, metrics, performance criteria, inflation trends, risk adjustment factors, attribution criteria and other factors. Revenue is recognized only when the price can be reasonably estimated and it is probable that a significant reversal will not occur once any uncertainty associated with the variable consideration is subsequently resolved. Shared savings revenue is recorded in the period under which the underlying services are provided during the pre-set twelve-month measurement period.
Care management
Under PMPM arrangements, the Company is paid a per member per month rate for each covered individual attributed by the payer to the Company (“attributed members”). Revenue is recognized in the month for which the PMPM rate applies and for which the member was attributed. The PMPM rate is based on a predetermined monthly contractual rate for each attributed member regardless of the volume of care coordination services provided under the contracts with the payers. The PMPM rate varies based on payer and product. Contingent PMPM amounts are not recognized into revenue until such contingency is resolved.
Revenue is reported at the amount that reflects the consideration to which the Company expects to be entitled in exchange for the provision of care coordination services to its population of attributed members. The Company’s contracts with payers have a single performance obligation that consists of a series of services for the provision of care coordination services for the population of attributed members for the duration of the contract. The transaction price for the contracts is variable, as it is primarily based on a PMPM rate on monthly attributed membership, which can fluctuate over the life of the contract.
The majority of the Company’s net PMPM transaction price relates specifically to the transfer of services for a distinct increment of the series and is recognized as revenue in the month in which attributed members are entitled to receive care coordination services.
Other Revenue
The remainder of the Company’s revenue is derived from leveraging the Company’s existing base of providers and patients to deliver value-oriented services including concierge services, virtual visits, virtual scribes and coding, clinical trials, behavioral health management, and partnerships with self-insured employers to offer direct primary care to their employees.
Fair Value of Financial Instruments
The Company’s financial instruments consist primarily of cash and cash equivalents, accounts receivable, other receivables and assets, accounts payable, and debt. The Company considers the carrying values of cash and cash equivalents, accounts receivable, other receivables, accounts payable, debt to related parties and debt to be indicative of their respective fair values. The carrying amount for debt approximates fair value which is defined as the price that would be received to sell an asset or paid to transfer a liability in an
orderly transaction between market participants at the measurement date. A three level hierarchy for fair value measurements is based upon the transparency of inputs to the valuation of an asset or liability as of the measurement date, defined as follows:
Level 1—inputs to the valuation methodology are quoted prices (unadjusted) for identical assets or liabilities in active markets.
Level 2—inputs to the valuation methodology include quoted prices for similar assets or liabilities in active markets, and inputs that are observable for the asset or liability, either directly or indirectly, for substantially the full term of the financial instrument.
Level 3—inputs to the valuation methodology are unobservable and significant to the fair value measurement.
A financial instrument’s categorization within the valuation hierarchy is based upon the lowest level of input that is significant to the fair value measurement. The Company’s financial instruments are classified as Level 1 assets and liabilities, as their fair values are based on unadjusted quoted prices in active markets for identical assets or liabilities.
Non-Controlling Interest
Non-controlling interest represents equity ownership that is not attributable to the Company. The consolidated financial statements include the assets, liabilities, revenues, and expenses of subsidiaries in which the Company has a controlling financial interest, including Privia Management Services Organization, LLC, Privia Management Company Montana, LLC, BASS Privia Management Company of California, LLC, Privia Management Company West Texas, LLC, Privia Management Company North Carolina, LLC, Privia Management Company of Ohio, LLC, Privia Services Company Connecticut, LLC, Privia Quality Network Connecticut, LLC, Privia Quality Network Delaware, LLC, our Owned Medical Groups, and Friendly Medical Groups. Net income attributable to non-controlling interests is separately presented in the consolidated statements of operations.
Income Taxes
The Company accounts for income taxes in accordance with the provisions of ASC Topic 740, Income Taxes (“ASC 740”). Under ASC 740, the Company follows the asset and liability method, which requires the recognition of deferred tax assets and liabilities for the expected future tax consequences of differences between the financial statement carrying amounts of assets and liabilities and their respective tax bases, as well as for operating loss and tax credit carryforwards.
Deferred tax assets and liabilities are measured using enacted tax rates expected to apply to taxable income in the years in which the temporary differences are expected to be recovered or settled. Under ASC 740, the effect on deferred tax assets and liabilities of a change in tax rates is recognized in income in the period that includes the enactment date. Should the Company determine that it is more likely than not that some portion or all of its deferred tax assets will not be realized, a valuation allowance to the deferred tax assets would be established in the period such determination was made. State corporate taxes were calculated based on a blended rate calculated based on the Company’s allocation and apportionment to the states. Calculation under the blended rate does not result in a material difference.
ASC 740 requires an entity to recognize the financial statement impact of a tax position when it is more likely than not that the position will be sustained upon examination. If the tax position meets the more likely than not recognition threshold, the tax effect is recognized at the largest amount of the benefit that has greater than a fifty percent likelihood of being realized upon ultimate settlement. ASC 740 also provides guidance for classification, interest and penalties, accounting in interim periods, disclosure, and transition. ASC 740 requires that a liability created for unrecognized tax benefits be presented as a separate liability and not combined with deferred tax liabilities or assets.
At December 31, 2025, and 2024, the Company believes it has appropriately accounted for any unrecognized tax benefits. To the extent the Company prevails in matters for which a liability for an unrecognized tax benefit is established or is required to pay amounts in excess of the liability, the Company’s effective tax rate in a given financial statement period may be affected. As there are no uncertain tax positions, the Company does not have any accrued interest or penalties associated with any unrecognized tax benefits. The Company and its subsidiaries file income tax returns in the U.S. federal jurisdiction and in various state jurisdictions. As of December 31, 2025, the periods subject to examination by the Company’s major jurisdictions (federal and various states) are generally for the years December 31, 2020 through December 31, 2024.
Provider Liability
Provider liability represents amounts payable to physicians, hospitals and other ancillary providers, including Privia Physicians, their related practices, as well as providers contracted through the Company’s payer arrangements. These liabilities include amounts not yet paid for physician guaranteed payments and other required distributions pursuant to the service agreements as well as medical claim costs for services provided to attributed beneficiaries for which the Company is financially responsible under at-risk capitated revenue arrangements whether paid directly by the Company or indirectly by payers with whom the Company has contracted.
Leases
The Company evaluates whether a contract is or contains a lease at the inception of the contract. Upon lease commencement, defined as the date on which a lessor makes the underlying asset available to the Company for use, the Company classifies the lease as either an operating or finance lease. The Company’s leases primarily consist of operating leases for office space in certain states in which the Company operates. The Company also has operating leases for equipment, which are not significant.
Right-of-use assets represent the Company’s right to use an underlying asset for the lease term and lease liabilities represent the Company’s obligation to make lease payments arising from the lease. Lease liabilities are measured at the present value of the remaining, fixed lease payments at lease commencement. The Company uses its incremental borrowing rate based on the information available at the later date of adoption, inception, or modification in determining the present value of lease payments. Right-of-use assets are measured at an amount equal to the initial lease liability, plus any prepaid lease payments (less any incentives received) and initial direct costs, at the lease commencement date. The Company has elected to account for lease and non-lease components as a single lease component for its facility leases. As a result, the fixed payments that would otherwise be allocated to the non-lease components are accounted for as lease payments and are included in the measurement of the Company’s right-of-use asset and lease liability. Lease expense for lease payments is recognized on a straight-line basis over the lease term and included in general and administrative expense within the accompanying consolidated statements of operations.
The Company does not recognize a lease liability or right-of-use asset within its consolidated balance sheets for short-term leases defined as a lease, that at its commencement date, has a term of 12 months or less and does not include a purchase option that the lessee is reasonably certain of exercise. Instead, short-term lease payments are recognized into expense on a straight-line basis over the lease term. When determining whether a lease qualifies as a short-term lease, the Company evaluates the lease term and the purchase option in the same manner as all other leases.
Provider Expense
Provider expense represents amounts accrued or payments made to physicians, hospitals and other service providers, including Privia Physicians, their related physician practices, and providers with whom the Company has contracted through payer partners. Those costs include physician guaranteed payments and other required distributions pursuant to the service agreements as well as medical claims costs for services provided to attributed beneficiaries under at-risk capitated revenue arrangements for which the Company is financially responsible whether paid directly by the Company or indirectly by payers with whom the Company has contracted. Provider expense is recognized in the period in which services are provided.
Cost of Platform
Cost of platform represents direct costs incurred to provide services to Privia Physicians and their practices. These costs include third-party electronic medical records and practice management software expenses, employee-related expenses, including salaries, employee benefits costs, stock-based compensation, consulting expenses, travel expenses and technology related costs for the team. Cost of platform excludes depreciation and amortization expense. Third-party electronic medical records and practice management software expenses are paid on a percentage of revenue basis, while employee-related expenses are variable based on the number of employees used to service the Company’s implemented physicians.
Sales and Marketing
Sales and marketing expense consists primarily of employee-related expenses, including salaries, stock-based compensation, commissions, and employee benefits for personnel engaged in marketing, sales, community outreach, and sales support. These expenses reflect the costs of both field-based and corporate sales and marketing teams. Sales and marketing expenses also include travel expenses and central and community-based advertising to drive awareness, engagement, and retention among current and prospective patients as well as the infrastructure required to support the Company’s marketing initiatives.
General and Administrative
Corporate, general and administrative expense includes employee-related expenses, including salaries, benefits and stock-based compensation, as well as expenses related to technology infrastructure, operations, clinical and quality support, finance, legal, human resources, and development departments. Additionally, general and administrative expense includes all corporate technology and occupancy costs.
Stock-Based Compensation
The Company accounts for share-based compensation in accordance with the provisions of ASC 718, Compensation–Stock Compensation (“ASC 718”), which requires the issuer to recognize compensation expense for all share-based payments made to employees based on the fair value of the share-based payment at the grant date. The Company estimates the fair value of stock options granted to employees and contractors using the Black-Scholes option-pricing model. Option valuation models require several inputs, such as the expected stock price volatility, the fair value of the stock, the risk free rate, the expected term of the award and the
dividend yield. The Company records share-based compensation forfeitures as a reversal of previously recognized compensation expense as the forfeitures occur. For additional information, refer to Note 11. “Stockholders’ Equity.”
The Company issues certain Performance Stock Unit (“PSU”) awards that vest upon satisfaction of specified service conditions, performance-based conditions, and/or market conditions. For some awards, the performance metrics have been identified; however, certain targets have not yet been established. For the awards with performance-based conditions where the target will be fully established at a future date, the Company has determined that the service inception date precedes the grant date for these awards as (a) the awards were authorized prior to establishing an accounting grant date, (b) the recipients began providing services prior to the grant date, and (c) there are performance conditions that, if not met by the accounting grant date, will result in the forfeiture of the awards. As the service inception date precedes the accounting grant date, stock-based compensation expense is recognized over the requisite service period based on the estimated fair value at each reporting date. For awards that are solely based on employment and the achievement of certain market performance metric targets, which have already been determined, the fair value of the PSUs is determined on the grant date using a Monte Carlo valuation model. Stock-based compensation expense for these awards is fixed and is recognized on a straight-line basis over the requisite service period.
Net Income per Share Attributable to Common Stockholders
Basic net income per share attributable to common stockholders is calculated by dividing the net income attributable to common stockholders by the weighted-average number of shares of common stock outstanding for the period.
Diluted net income per share attributable to common stockholders is calculated by dividing net income attributable to common stockholders by the weighted-average number of common shares outstanding during the period, including the effect of dilutive common stock equivalents, determined using the treasury stock method. Dilutive securities are excluded from diluted earnings per share in periods in which their inclusion would be antidilutive.
Recently Adopted Accounting Pronouncements
In December 2023, the FASB issued Accounting Standards Update (“ASU”) No. 2023-09, Income Taxes - Improvements to Income Tax Disclosures (“ASU 2023-09”). The amendments require (i) enhanced disclosures in connection with an entity's effective tax rate reconciliation and (ii) income taxes paid disaggregated by jurisdiction. The amendment is effective for annual periods beginning after December 15, 2024. The Company adopted ASU 2023-09 for the annual period ending December 31, 2025 on a prospective basis. See Note 10. “Income Taxes” for the related disclosures.
Recently Issued Accounting Pronouncements Pending Adoption
In November 2024, the FASB issued ASU No. 2024-03, Disaggregation of Income Statement Expenses (“DISE”) (“ASU 2024-03”). The amendments require disclosures about the nature of expenses included in the income statement, such as purchases of inventory, employee compensation and depreciation. The amendment is effective for annual reporting periods beginning after December 15, 2026, and interim reporting periods beginning after December 15, 2027. The Company is currently evaluating the impact of ASU 2024-03 on its financial statements and related disclosures.
In May 2025, the FASB issued ASU No. 2025-03, Business Combinations (Topic 805) and Consolidation (Topic 810): Determining the Accounting Acquirer in a Variable-Interest Entity. The amendment clarifies the guidance when an entity involved in an acquisition transaction effected primarily by exchanging equity interests and the legal acquiree is a VIE that meets the definition of a business. Entities must identify the accounting acquirer using the factors in ASC 805-10-55-12 through 55-15, rather than relying solely on the VIE consolidation model. The amendment is effective for annual reporting periods beginning after December 15, 2026, including interim periods within the fiscal years and applied prospectively to acquisitions after the adoption date. The Company is currently evaluating the impact of this standard on its financial statements and related disclosures.
In July 2025, the FASB issued ASU No. 2025-05, Financial Instruments — Credit Losses (Topic 326): Measurement of Credit Losses for Accounts Receivable and Contract Assets (“ASU 2025-05”), which provides a practical expedient for estimating expected credit losses for current accounts receivable and current contract assets. The amendment is effective for annual reporting periods beginning after December 15, 2025, including interim periods within the fiscal years and applied prospectively after the adoption date. The Company does not expect ASU 2025-05 to have a material impact on its financial statements and related disclosures.
2. Revenue Recognition
The following table presents the Company’s revenues disaggregated by source:
| | | | | | | | | | | | | | | | | |
| For the Years Ended December 31, |
| (Dollars in Thousands) | 2025 | | 2024 | | 2023 |
| FFS-patient care | $ | 1,360,235 | | | $ | 1,146,156 | | | $ | 976,688 | |
| FFS-administrative services | 137,017 | | | 125,431 | | | 113,154 | |
| Capitated revenue | 308,458 | | | 212,987 | | | 338,729 | |
| Shared savings | 234,815 | | | 179,202 | | | 170,143 | |
| Care management fees (PMPM) | 73,138 | | | 64,066 | | | 50,519 | |
| Other revenue | 9,179 | | | 8,548 | | | 8,504 | |
| Total Revenue | $ | 2,122,842 | | | $ | 1,736,390 | | | $ | 1,657,737 | |
| | | | | |
FFS-patient care is primarily generated from third-party payers with which the Company has established contractual billing arrangements. The following table presents the approximate percentages by source of net revenue received for healthcare services provided for the periods indicated:
| | | | | | | | | | | | | | | | | |
| For the Years Ended December 31, |
| 2025 | | 2024 | | 2023 |
| Commercial insurers | 71 | % | | 71 | % | | 70 | % |
| Government payers | 15 | % | | 14 | % | | 15 | % |
| Patient | 14 | % | | 15 | % | | 15 | % |
| 100 | % | | 100 | % | | 100 | % |
FFS-administrative services revenue is earned through the Company’s MSA with Non-Owned Medical Groups primarily based on a fixed percentage of net collections from patient care generated by those medical groups.
VBC revenue is primarily earned through contracts that include Capitated revenue, Shared savings and Care management fees. Capitated revenue is generated from “at-risk contracts” under which the Company receives a fixed monthly payment from third-party payers in exchange for providing healthcare services to attributed beneficiaries. The Company is responsible for delivering or covering the cost of required healthcare services attributed to these beneficiaries. At-risk Capitated revenue is recorded gross in revenues as the Company acts as the principal in arranging, providing, and controlling managed healthcare services provided to the attributed lives. Shared savings revenue and Care management fees are generated through contracts with large commercial payer organizations and the U.S. Federal Government.
For shared savings arrangements, the Company estimates the transaction price by analyzing the activities during the relevant time period in consideration of the agreed-upon benchmarks, metrics, performance criteria, inflation trends, risks adjustment factors, attribution criteria and any other contractually defined factors. Revenue is recognized only when the transaction price can be reasonably estimated and it is probable that a significant reversal will not occur, once uncertainties related to the variable consideration are resolved. Revenue is recorded over the period in which services are provided, typically during a pre-set twelve-month measurement period. Subsequent changes to the estimated transaction price are generally recorded as adjustments to revenue in the period of the change. In September 2025, the Company received final settlement notices from CMS for the Company’s portion of MSSP shared savings generated during the 2024 performance year. For the year ended December 31, 2025, the amount of revenue recognized related to the change in estimate of our Shared Savings accrual was $28.5 million.
Contract Asset
The Company has the following contract assets:
| | | | | | | | | | | |
| (Dollars in Thousands) | December 31, 2025 | | December 31, 2024 |
| Balances for contracts with customers | | | |
Accounts receivable, net | $ | 400,902 | | | $ | 316,179 | |
| | | |
Remaining Performance Obligations
The Company does not disclose the value of the remaining performance obligations or the expected timing of revenue recognition at the end of the reporting period as it has minimal unsatisfied performance obligations. Patients generally have no obligation to continue receiving services at the Company’s facilities and substantially all performance obligations are satisfied at the time the service is rendered.
3. Business Combinations
2025 Acquisitions
Arizona
In April 2025, the Company entered the Arizona market with the acquisition of a 51% ownership interest in PMG AZ. The acquisition was accounted for using the acquisition method pursuant to the requirements of ASC 805. The results of operations and cash flows for the period subsequent to the acquisition are included in the accompanying consolidated statement of operations and consolidated statement of cash flows.
The preliminary fair value of the assets acquired and liabilities assumed at the acquisition date are as follows (in thousands):
| | | | | | | | |
Cash | | $ | 5,942 | |
Accounts receivable | | 6,319 | |
Identifiable intangible assets: | | |
| Payer contract and physician network intangibles | | 64,400 | |
| Goodwill | | 43,838 | |
Deferred tax liabilities | | (13,238) | |
Provider liability | | (12,261) | |
| Total acquired net assets | | $ | 95,000 | |
Information regarding the net cash paid for the acquisition is as follows (in thousands):
| | | | | | | | |
Fair value of assets acquired, net of $5.9 million of cash acquired | | $ | 70,719 | |
Provider liability | | (12,261) | |
Deferred tax assets | | (13,238) | |
| Goodwill | | 43,838 | |
Net cash paid for acquisition | | $ | 89,058 | |
In connection with the 2025 transaction related to PMG AZ, the seller is entitled to additional amounts up to a maximum value of $25.0 million, subject to meeting certain future targets. Of the $25.0 million, $10.0 million may be earned over a three-year period beginning at the acquisition date, and $15.0 million may be earned upon renewal of certain agreements in 2030. The Company accounted for these additional amounts as post combination expense and expects to recognize any amounts earned within General and administrative expenses in the consolidated statements of operations and Accounts payable and accrued expenses and Other non-current liabilities, for current and long-term liabilities, respectively, within the consolidated balance sheets.
During the year ended December 31, 2025, a measurement period adjustment was recorded to offset deferred tax assets, thereby increasing goodwill by $1.7 million. The goodwill relating to this acquisition is primarily attributable to synergies related to the assembled workforce. None of the goodwill recognized for the acquisition of PMG AZ is expected to be deductible for tax purposes. The Company is in the process of completing its final valuation analysis to identify and determine the fair value of tangible and identifiable intangible assets acquired and the liabilities assumed. Thus, the final allocation of the purchase price may differ from the preliminary estimates used at December 31, 2025 based on additional information obtained and completion of the valuation of the identifiable intangible assets.
Evolent
In December 2025, the Company acquired an ACO business from Evolent Health, Inc. (“Evolent”). The accompanying consolidated balance sheet includes the preliminary estimated fair values of the net assets acquired. The results of operations and cash flows for the period subsequent to the acquisition are included in the accompanying consolidated statement of operations and consolidated statement of cash flows.
The preliminary fair value of the assets acquired and liabilities assumed at the acquisition date were as follows (in thousands):
| | | | | | | | |
| | |
Accounts receivable | | $ | 29,515 | |
Identifiable intangible assets: | | |
Payer contract | | 50,880 | |
| Goodwill | | 24,389 | |
Provider liability | | (13,472) | |
| Total acquired net assets | | $ | 91,312 | |
Information regarding the net cash paid for the acquisition is as follows (in thousands):
| | | | | | | | |
Fair value of assets acquired | | $ | 80,395 | |
Provider liability | | (13,472) | |
| Goodwill | | 24,389 | |
Net cash paid for acquisition | | $ | 91,312 | |
In connection with the 2025 transaction related to Evolent, the seller is entitled to additional consideration up to $13.0 million if certain conditions are met. The Company has recognized the acquisition-date fair value of the contingent consideration of $2.9 million and determined the liability to be a Level 3 instrument due to significant inputs that are not observable in the market. The fair value of the contingent consideration was calculated based on the income approach. The expected (probability-weighted) payment amount is estimated based on the likelihood of achieving the threshold and target levels. The present value of the expected payment was calculated by discounting the expected payment amount from the expected payment date to the valuation date, at an appropriate discount rate. The amount will be remeasured and adjusted quarterly, if necessary, based on the assessed fair value.
The goodwill relating to this acquisition is primarily attributable to synergies related to the assembled workforce. All of the goodwill recognized for the acquisition of Evolent is expected to be deductible for tax purposes. The Company is in the process of completing its final valuation analysis to identify and determine the fair value of tangible and identifiable intangible assets acquired and the liabilities assumed. Thus, the final allocation of the purchase price may differ from the preliminary estimates used at December 31, 2025 based on additional information obtained and completion of the valuation of the identifiable intangible assets.
In December 2025, the Company acquired 51% of Privia Medical Group Florida, LLC from Health First Medical Group, LLC.
Pro Forma Total Revenues
The 2025 acquisitions contributed revenues of $51.9 million from the date of acquisition through December 31, 2025. The following table summarizes the unaudited pro forma total revenues of the combined entity had the date of the acquisition been January 1, 2024:
| | | | | | | | | | | | | | | | | |
(unaudited) | | | For the Twelve Months Ended December 31, |
| (Dollars in Thousands) | | | | | 2025 | | 2024 |
| Pro forma combined entity total revenue | | | | | $ | 2,311,149 | | | $ | 1,970,772 | |
2024 Acquisitions
In January 2024, PMG West Texas Holdings, PLLC, a Nominee PC, acquired a majority ownership interest in an independent physician association in the Gulf Coast Market. The Company, through one of its affiliates, is a party to a Restriction Agreement with the Nominee PC. The results of operations of the acquisition are included in the Company’s consolidated financial statements since the acquisition date.
In November 2024, the Company acquired Privia Medical Group Indiana, LLC, (“PMG IN”). PMG IN is a physician-owned Medical Group, with PMG Indiana Holdings, LLC (“Friendly IN PC”), an Indiana professional limited liability company wholly owned by a licensed physician with a leadership role in the Company, holding a majority membership interest and having governance and control rights pursuant to the governing documents of PMG IN. The Company has a contractual relationship with Friendly IN PC through a Restriction Agreement. Friendly IN PC owns 51% interest in PMG IN. The results of operations of the acquisition have been included in the Company’s consolidated financial statements since the acquisition date.
The purchase price for the acquisitions noted above was allocated as follows:
| | | | | | | | | | |
| (Dollars in thousands) | | | | For the Year Ended December 31, 2024 |
| Cash paid, net of cash acquired | | | | $ | 6,957 | |
| Contingent payables | | | | 4,250 | |
| Total consideration | | | | $ | 11,207 | |
| | | | |
| | | | |
| | | | |
| | | | |
| Payer contract and physician network intangibles | | | | $ | 8,342 | |
| | | | |
| | | | |
| | | | |
| Goodwill | | | | 2,865 | |
| | | | |
| Total acquired net assets | | | | $ | 11,207 | |
The goodwill relating to these acquisitions is primarily attributable to synergies related to the assembled workforce. Goodwill is measured as the excess of the consideration transferred over the fair value of the net assets acquired on the acquisition date.
4. Goodwill and Intangible Assets, Net
For the purposes of the goodwill impairment assessment, the Company as a whole is one reporting unit as the Chief Operating Decision Maker (“CODM”) reviews financial results on a consolidated basis. The Company recognizes the excess of the purchase price, plus the fair value of any non-controlling interests in the acquiree, over the fair value of identifiable net assets acquired as goodwill. The Company performs a qualitative assessment on goodwill at least annually or more frequently if events or changes in circumstances indicate that the carrying value of goodwill may not be recoverable. If it is determined in the qualitative assessment that the fair value of a reporting unit is more likely than not below its carrying amount, then the Company will perform a quantitative impairment test. The quantitative goodwill impairment test is performed by comparing the fair value of a reporting unit with its carrying amount. Any excess in the carrying value of a reporting unit’s goodwill over its fair value is recognized as an impairment loss, limited to the total amount of goodwill allocated to that reporting unit. The carrying value of goodwill at December 31, 2025 and 2024 is $209.8 million and $141.6 million, respectively. No indicators of impairment were identified during the years ended December 31, 2025, 2024, and 2023. As of December 31, 2025, there was no accumulated impairment of goodwill.
During January 2024, PMG West Texas Holdings, PLLC, a Nominee PC, acquired a majority ownership interest in an independent physician association in the Gulf Coast Market. The Company, through one of its affiliates, is party to a Restriction Agreement with the Nominee PC. The Company recorded Goodwill of $0.7 million in connection with the acquisition, representing the excess of the purchase price over the fair value of the net assets acquired.
During November 2024, the Company entered into the Indiana market through the acquisition of Privia Medical Group Indiana, LLC (“PMG IN”), whereby Privia acquired majority ownership in PMG IN. The Company recorded Goodwill of $2.2 million in connection with PMG IN, which represents the excess of the purchase price over the fair value of the net assets acquired.
During April 2025, the Company entered into the Arizona market through the acquisition of PMG AZ, whereby Privia acquired a 51% ownership interest in PMG AZ. During the year ended December 31, 2025, the Company recorded Goodwill of $43.8 million in connection with PMG AZ, which represents the excess of the purchase price over the fair value of the net assets acquired.
During December 2025, the Company acquired an ACO business from Evolent Health, Inc. In this connection, the Company recorded Goodwill of $24.4 million, which represents the excess of the purchase price over the fair value of the net assets acquired.
A summary of the Company’s intangible assets is as follows:
| | | | | | | | | | | | | | | | | | | | | | | |
| December 31, 2025 | | December 31, 2024 |
| (Dollars in thousands) | Intangible
Assets | | Accumulated
Amortization | | Intangible
Assets | | Accumulated
Amortization |
| Trade names | $ | 4,600 | | | $ | 2,607 | | | $ | 4,600 | | | $ | 2,377 | |
| Consumer customer relationships | 3,100 | | | 2,783 | | | 3,100 | | | 2,758 | |
| Management Service Agreement | 2,200 | | | 1,409 | | | 2,200 | | | 1,272 | |
| Physician network | 16,052 | | | 2,016 | | | 10,902 | | | 916 | |
| Payer contracts | 167,443 | | | 9,978 | | | 57,313 | | | 4,768 | |
| MSO Service Agreement | 51,800 | | | 10,483 | | | 51,800 | | | 8,017 | |
| 245,195 | | | $ | 29,276 | | | 129,915 | | | $ | 20,108 | |
| Less accumulated amortization | (29,276) | | | | | (20,108) | | | |
| Intangible assets, net | $ | 215,919 | | | | | $ | 109,807 | | | |
The remaining weighted average life of all amortizable intangible assets is approximately 17.5 years at December 31, 2025.
Amortization expense for intangible assets was approximately $9.2 million, $6.2 million and $5.4 million for the years ended December 31, 2025, 2024, and 2023, respectively.
Remaining estimated amortization expense for the Company’s intangible assets is as follows:
| | | | | |
| (Dollars in Thousands) |
| 2026 | $ | 12,541 | |
| 2027 | 12,541 | |
| 2028 | 12,541 | |
| 2029 | 12,541 | |
| 2030 | 12,541 | |
| Thereafter | 153,214 | |
| Total | $ | 215,919 | |
5. Leases
The Company leases office space under various operating lease agreements. The initial terms of these leases range from 3 to 9 years and generally provide for periodic rent increases and renewal options.
The components of lease expense were as follows:
| | | | | | | | | | | | | | |
| (Dollars in Thousands) | | For the Years Ended December 31, |
| | 2025 | | 2024 |
| Operating lease cost | | $ | 3,157 | | $ | 2,772 |
| | | | |
| Cash paid for amounts included in the measurement of lease liabilities - operating leases | | $ | 2,371 | | $ | 2,888 |
| Weighted-average remaining lease term - operating leases | | 4.8 Years | | 3.1 Years |
| Weighted-average discount rate - operating leases | | 3.9 | % | | 2.6 | % |
| | | | |
| | | | |
The aggregate future lease payments for operating leases in the years subsequent to December 31, 2025 are as follows:
| | | | | | | | |
| (Dollars in Thousands) | | |
| 2026 | | $ | 2,141 | |
| 2027 | | 2,196 | |
| 2028 | | 1,874 | |
| 2029 | | 1,681 | |
| 2030 | | 1,646 | |
| Thereafter | | 1,073 | |
| Total future lease payments | | 10,611 | |
| Imputed interest | | (1,080) | |
| Total | | $ | 9,531 | |
6. Property and Equipment, Net
A summary of the Company’s property and equipment, net is as follows:
| | | | | | | | | | | |
| (Dollars in Thousands) | December 31, 2025 | | December 31, 2024 |
| Furniture and fixtures | $ | 1,402 | | | $ | 1,402 | |
| Computer equipment | 1,686 | | | 1,686 | |
| Leasehold improvements | 4,960 | | | 4,960 | |
| 8,048 | | | 8,048 | |
| Less accumulated depreciation and amortization | (7,544) | | | (6,806) | |
| Property and equipment, net | $ | 504 | | | $ | 1,242 | |
Depreciation and amortization expense for property and equipment was approximately $0.7 million, $1.1 million and $1.2 million for the years ended December 31, 2025, 2024, and 2023, respectively.
7. Account Payable and Accrued Expenses
Accounts payable and accrued expenses consist of the following:
| | | | | | | | | | | |
| (Dollars in Thousands) | December 31, 2025 | | December 31, 2024 |
| Accounts payable | $ | 7,973 | | | $ | 9,755 | |
| Accrued employee compensation and benefits | 33,552 | | | 26,420 | |
| Other accrued expenses | 55,279 | | | 45,811 | |
| Total accounts payable and accrued expenses | $ | 96,804 | | | $ | 81,986 | |
8. Provider Liability
Provider liability represents amounts payable to physicians, hospitals and other ancillary providers, including both Privia physicians (and their related physician practices), and providers the Company has contracted with through payer partners. These liabilities include amounts not yet paid for physician guaranteed payments and other required distributions pursuant to the service agreements as well as medical claims costs for services provided to attributed beneficiaries for which the Company is financially responsible under at-risk Capitated revenue arrangements, whether paid directly by the Company or indirectly by payers with whom the Company has contracted. Provider expense is recognized in the period in which services are provided and include estimates of claims that have been incurred but have either not yet been received, processed, or paid and as such, not reported.
The Company’s provider liability balance represents management’s best estimate of its obligation for unpaid provider expenses. Management exercises judgment to determine the assumptions used for developing the required estimates. Provider liability estimates are developed using actuarial methods commonly used by health insurance actuaries that include a number of factors and assumptions including medical service utilization trends, changes in membership, observed medical cost trends, historical claim payment patterns and other factors.
Periodically, the Company re-examines previously established provider liability estimates based on actual claim submissions and other changes in facts and circumstances. The Company adjusts its provider liability estimates as more complete claims information becomes available, recognizing changes in the period in which they are identified. Differences between estimated liabilities and actual claim settlements are recognized in the period the claims are settled.
Liabilities for unpaid medical claims under at-risk capitation arrangements, included in Provider liability in the accompanying consolidated balance sheets, are as follows:
| | | | | | | | | | | | | | |
(Dollars in Thousands) | | December 31, 2025 | | December 31, 2024 |
Balance, beginning of period | | $ | 66,355 | | | $ | 67,138 | |
| Incurred health care costs: | | | | |
| Current year | | 303,075 | | | 208,341 | |
| Prior years | | (12,617) | | | 964 | |
Total claims incurred | | 290,458 | | | 209,305 | |
| Claims paid: | | | | |
| Current year | | (232,079) | | | (157,375) | |
| Prior year | | (45,745) | | | (52,713) | |
| Total claims paid | | (277,824) | | | (210,088) | |
| | | | |
| | | | |
Balance, end of period | | $ | 78,989 | | | $ | 66,355 | |
9. Debt
On November 16, 2023, Privia Health Group, Inc., PH Group Holdings Corp., and Privia Health, LLC, as borrower, (collectively, the “Privia Parties”) entered into a credit agreement (the “Revolving Credit Agreement”) with Wells Fargo Bank, National Association, as issuing lender, and certain other lenders, with borrowing availability of revolving loans and letters of credit up to $125 million (the “Revolving Credit Facility”). The Revolving Credit Facility is senior secured, expires in November 2028 and bears interest at either i) a base rate, as defined, plus an applicable margin ranging from 0.25% to 0.75%, or ii) Secured Overnight Financing Rate (“SOFR”) plus 0.10%, plus an applicable margin that ranges from 1.25% to 1.75%, depending on the consolidated leverage ratio, as defined. The Revolving Credit Facility includes a commitment fee on the unused Revolving Credit Facility that ranges from 0.20% to 0.30% (0.20% per annum at year end) depending on the consolidated leverage ratio, as defined. The facility generally may be used for capital expenditures, expenses related to transactions and general corporate purposes.
The Revolving Credit Agreement contains customary affirmative, negative and financial covenants, and events of default. The occurrence of an event of default under the Revolving Credit Agreement may cause the unpaid principal and accrued interest, and all other obligations under the Revolving Credit Agreement to become immediately due and payable.
As of December 31, 2025, no amounts were outstanding under the Revolving Credit Facility. Substantially all of the Company’s real and personal property serve as collateral under this agreement.
10. Income Taxes
The provision for income taxes for years ending December 31, 2025, 2024, and 2023 are as follows: | | | | | | | | | | | | | | | | | |
| December 31, |
| (Dollars in Thousands) | 2025 | | 2024 | | 2023 |
Current: | | | | | |
| Federal | $ | 1,707 | | | $ | 1,022 | | | $ | — | |
| State and local | 1,634 | | | 987 | | | 528 | |
| Total current income tax expense | 3,341 | | | 2,009 | | | 528 | |
| | | | | |
| Deferred: | | | | | |
| Federal | $ | 9,460 | | | $ | 7,234 | | | $ | 6,221 | |
| State and local | 1,411 | | | 1,583 | | | 1,244 | |
| Total deferred income tax expense | 10,871 | | | 8,817 | | | 7,465 | |
| Total income tax expense | $ | 14,212 | | | $ | 10,826 | | | $ | 7,993 | |
Deferred taxes reflect the net tax effects of temporary differences between the carrying amounts of assets and liabilities for financial reporting purposes and the amounts used for income tax purposes. Deferred tax assets and deferred tax liabilities as of December 31, 2025, and 2024 are as follows:
| | | | | | | | | | | |
| (Dollars in Thousands) | December 31, 2025 | | December 31, 2024 |
Deferred tax assets | | | |
| Net operating loss carryforwards | $ | 6,896 | | | $ | 11,537 | |
| Stock compensation | 21,099 | | | 22,994 | |
| Lease liability | 2,506 | | | 1,774 | |
| Other accruals | — | | | 73 | |
| Total gross tax assets | 30,501 | | | 36,378 | |
| Less: valuation allowance | — | | | — | |
| Total deferred tax assets | $ | 30,501 | | | $ | 36,378 | |
| | | |
Deferred tax liabilities | | | |
Fixed and intangible assets | $ | (24,482) | | | $ | (8,698) | |
Right-of-use assets | (2,219) | | | (1,297) | |
Other | (1,526) | | | — | |
Total deferred tax liabilities | (28,227) | | | (9,995) | |
Deferred tax assets, net | $ | 2,274 | | | $ | 26,383 | |
For the years ended December 31, 2025, and 2024, the Company completed an assessment of the likelihood of realizing all or some portion of its net deferred tax assets. Based on an analysis of the positive and negative evidence, the Company determined it was more likely than not that the Company will be in a position to realize the benefits of the deferred tax asset as a result of consistent profitability. As such, no valuation allowance was recorded in either year. As of December 31, 2025, the Company has remaining federal and state net operating loss carryforwards of approximately $26.9 million and $24.7 million (post-apportioned state NOL) respectively, that begin to expire in 2035.
The following is a reconciliation of income tax computed at the U.S. federal statutory income tax rate to the provision for income taxes for the year ended December 31, 2025:
| | | | | | | | | | | |
| | Dollars | Rate |
| (Dollars in Thousands) | December 31, 2025 |
United States federal statutory rate | $ | 9,227 | | | 21.0 | % |
State and Local income taxes, net of federal income tax effect | 2,757 | | | 6.3 | |
Nontaxable or nondeductible items | | | |
Share-based payment awards | 2,867 | | | 6.5 | |
| Non-controlling interest | (1,430) | | | (3.3) | |
Other | 330 | | | 0.8 | |
Other adjustments | 461 | | | 1.0 | |
Provision for income taxes | $ | 14,212 | | | 32.3 | % |
The following is a reconciliation of income tax computed at the U.S. federal statutory income tax rate to the provision for income taxes for the years ended December 31, 2024, and 2023:
| | | | | | | | | | | | | | | | | | | | | | | | | | | | | |
| | | |
| | Dollars | | Rate |
| (Dollars in Thousands) | | 2024 | | 2023 | | | 2024 | | 2023 |
Tax provision computed at federal statutory income tax rate | | $ | 6,041 | | | $ | 6,094 | | | | 21.0 | % | | 21.0 | % |
Stock compensation | | 3,136 | | | (22) | | | | 10.9 | | | (0.1) | |
State tax expense, net of federal benefit | | 2,051 | | | 2,140 | | | | 7.1 | | | 7.4 | |
| | | | | | | | | |
Rate change | | 97 | | | (115) | | | | 0.3 | | | (0.4) | |
| Non-controlling interest | | (486) | | | 331 | | | | (1.7) | | | 1.1 | |
Other | | (13) | | | (435) | | | | — | | | (1.5) | |
Provision for income taxes | | $ | 10,826 | | | $ | 7,993 | | | | 37.6 | % | | 27.5 | % |
The stock compensation impacting the income tax provision is primarily attributable to stock-based compensation expense that is not deductible under Section 162(m), partially offset by tax deductible stock-based compensation.
The 2020 through 2024 federal and state income tax returns are within the statute of limitations and are currently not under examination by any federal or state tax authority.
The Company assesses the uncertainty in its income tax positions to determine whether a tax position of the Company is more likely than not to be sustained upon examination, including resolution of any related appeals of litigation processes, based on the technical merits of the position. For the tax position meeting the more-likely-than-not threshold, the tax amount recognized in the financial statements is reduced by the largest benefit that has a greater than 50% likelihood of being realized upon the ultimate settlement with the relevant taxing authority. As of December 31, 2025, and 2024, the Company had not recorded any reserves for uncertain tax positions or related interest and penalties.
The following is a reconciliation of the income taxes paid (net of refunds received) for the year ended December 31, 2025:
| | | | | |
| | |
| Jurisdiction | Income Taxes Paid (net of refunds received) |
(Dollars in Thousands) |
U.S. Federal | $ | 4,900 | |
States | 1,739 | |
Total | $ | 6,639 | |
11. Stockholders’ Equity
2021 Omnibus Incentive Plan
On April 6, 2021, the Board approved the 2021 Omnibus Incentive Plan (the “Plan”) which permits awards in respect of up to 10,278,581 shares of Common Stock. The Plan also provides for an automatic increase on the first day of each fiscal year following the effective date of the Plan by an amount equal to the lesser of (i) 5% of outstanding shares on December 31 of the immediately preceding fiscal year or (ii) such number of shares as determined by the Company’s Compensation Committee in its discretion. As of December 31, 2025, the Board has authorized 22,215,088 shares for issuance under the Plan. The Plan provides for the granting of stock options at a price equal to at least 100% of the fair market value of Common Stock as of the date of grant. The Plan also provides for the granting of Stock Appreciation Rights, Restricted Stock, Restricted Stock Units (“RSUs”), PSUs and other cash-based
or other stock-based awards, all of which must be granted at not less than the fair market value of Common Stock as of the date of grant.
Prior to the Company’s initial public offering (“IPO”), the Company granted stock options pursuant to the PH Group Parent Corp. Stock Option Plan (the “PH Parent Option Plan”). The Company no longer issues grants under the PH Parent Option Plan and no shares of Common Stock are reserved for future issuance thereunder.
2021 Employee Stock Purchase Plan
In April 2021, the Board of Directors approved the Company’s 2021 Employee Stock Purchase Plan (“2021 ESPP”). The 2021 ESPP became effective upon the execution of the underwriting agreement for the Company’s IPO in April 2021. Per the 2021 ESPP, shares may be newly issued shares, treasury shares or shares acquired on the open market. The Compensation Committee may elect to increase the total number of shares available for purchase under the 2021 ESPP as of the first day of each Company fiscal year following the effective date of the 2021 ESPP in an amount equal to up to one percent (1%) of the shares issued and outstanding on the immediately preceding December 31; provided that the maximum number of shares that may be issued under the Plan in any event shall be 10,278,581 shares. As of the date of the IPO, the Company has reserved 1,027,858 shares of common stock for issuance under the 2021 ESPP. As of December 31, 2025, no shares have been issued under this plan.
Novant Health Private Placement
On March 2, 2023, the Company entered into a strategic alignment agreement (the “Equity Alignment Agreement”) with ChoiceHealth, Inc. (“Novant Sub”), a subsidiary of Novant Health, Inc. (“Novant Health”), in connection with the strategic partnership between the Company and Novant Health entered into in November 2022 to launch Privia Medical Group — North Carolina.
Pursuant to the Equity Alignment Agreement, Novant Sub will be entitled to receive, and the Company agreed to issue, shares of the Company’s common stock, par value $0.01 per share (the “Common Stock”), to Novant Sub any time each of the following events occurs, in the following amounts:
1.The Company will issue 745,712 shares of Common Stock to Novant Sub each time Privia Medical Group — North Carolina implements 1,000 providers in specified markets in North Carolina.
2.The Company will issue 372,856 shares of Common Stock to Novant Sub each time the Company and Novant Health enter a new state pursuant to a mutually agreed business plan developed for such state.
3.The Company will issue 745,712 shares of Common Stock to Novant Sub each time the partnership between the Company and Novant Health for each new state implements 1,000 providers in specified core markets in such state.
The Equity Alignment Agreement will renew every four years, subject to the delivery of a third-party valuation opinion. The renewal will be required to use the same issuance events, but the number of shares may be adjusted to be consistent with the valuation opinion. The total number of shares of Common Stock issuable to Novant Sub under the Equity Alignment Agreement and all renewals of the Equity Alignment Agreement are subject to a total cap equal to 19.9% of the total number of shares of Common Stock outstanding as of the effective date of the Equity Alignment Agreement and as of the effective date of all renewals, whichever is lowest. No shares have been issued to Novant Sub under the Equity Alignment Agreement as of December 31, 2025. A member of the Board is a member of the board of trustees of Novant Health.
Stock option activity
The fair value of stock options issued under the Plan is calculated using a Black-Scholes option pricing model that requires several inputs, including expected stock price volatility, the fair value of the underlying common stock, the risk-free interest rate, expected term of the award and dividend yield. The Company estimated the inputs as follows:
•Volatility is based on the Company’s historical common stock volatility since inception.
•Fair value of common stock is the publicly quoted price on Nasdaq.
•The risk-free interest rate is the implied yield available on U.S. Treasury zero-coupon issues with an equivalent expected term of the option.
•The expected term is the period that the Company’s stock-based awards are expected to be outstanding. The expected term assumption is based on the simplified method in which the expected term is equal to the average of the stock-based award’s weighted-average vesting period and its contractual term. The Company expects to continue using the simplified method until sufficient information about historical behavior is available.
•Dividend yield is zero, as the Company has not declared or paid any cash dividend and does not currently plan to pay a cash dividend in the foreseeable future.
The following table summarizes stock option activity under the PH Parent Option Plan and Plan:
| | | | | | | | | | | | | | | | | | | | | | | |
| Number of Shares | | Weighted-
Average
Exercise Price | | Weighted- Average Remaining Contractual Life (Years) | | Aggregate Intrinsic
Value
(in thousands) |
Outstanding at January 1, 2023 | 13,176,721 | | | $ | 7.86 | | | 9.02 | | $ | 197,695 | |
| Granted | — | | | — | | | | | |
| Exercised | (3,104,257) | | | 2.82 | | | | | |
| Forfeited | (251,710) | | | 22.78 | | | | | |
Outstanding at December 31, 2023 | 9,820,754 | | | $ | 9.06 | | | 7.90 | | $ | 138,028 | |
| Granted | — | | | — | | | | | |
| Exercised | (1,259,513) | | | 2.08 | | | | | |
| Forfeited | (34,331) | | | 24.50 | | | | | |
Outstanding at December 31, 2024 | 8,526,910 | | | $ | 10.03 | | | 7.17 | | $ | 93,074 | |
| Granted | — | | | — | | | | | |
| Exercised | (973,513) | | | 8.10 | | | | | |
| Forfeited | (18,732) | | | 21.34 | | | | | |
Balance at December 31, 2025 | 7,534,665 | | | $ | 10.26 | | | 6.28 | | $ | 102,102 | |
| Exercisable at December 31, 2025 | 7,511,216 | | | $ | 10.21 | | | 6.28 | | $ | 102,102 | |
RSU Activity
The following table summarizes the RSU activity under the Plan:
| | | | | | | | | | | |
| Number of Shares | | Grant Date Fair Value |
Outstanding at January 1, 2023 | 2,404,664 | | | $ | 23.81 | |
| Granted | 1,161,301 | | | 27.50 | |
| Vested | (425,076) | | | 24.11 | |
| Forfeited | (193,787) | | | 24.43 | |
Unvested and outstanding at December 31, 2023 | 2,947,102 | | | $ | 25.18 | |
| Granted | 2,203,174 | | | 22.55 | |
| Vested | (815,637) | | | 25.69 | |
| Forfeited | (192,364) | | | 23.85 | |
Unvested and outstanding at December 31, 2024 | 4,142,275 | | | $ | 23.73 | |
| Granted | 2,223,500 | | | 24.85 | |
| Vested | (2,318,016) | | | 23.67 | |
| Forfeited | (200,576) | | | 24.23 | |
| Unvested and outstanding at December 31, 2025 | 3,847,183 | | | $ | 24.39 | |
PSU Activity
PSUs granted under the Plan generally vest based on the satisfaction of specified service conditions, performance-based conditions, and/or market conditions. PSUs represent a target number of units that may be paid out at zero to 200% of target at the end of a multi-year award cycle, typically three years, subject to continued employment of recipients and the achievement of such performance-based and market conditions. The performance-based conditions are established relative to certain Company-specific financial targets. For PSUs with performance-based conditions where the target will be fully established at a future date, the Company has determined that the service inception date precedes the grant date for these awards as (a) the awards were authorized prior to establishing an accounting grant date, (b) the recipients began providing services prior to the grant date, and (c) there are performance conditions that, if not met by the accounting grant date, will result in the forfeiture of the awards. As the service inception date precedes the accounting grant date, stock-based compensation expense is recognized over the requisite service period based on the estimated fair value at each reporting date. For PSUs that are solely based on employment and the achievement of certain market performance metric targets, which have already been determined, the fair value of the PSUs is determined on the grant date using a Monte Carlo valuation model. Stock-based compensation expense for these awards are fixed and is recognized on a straight-line basis over the requisite service period. At the end of the performance period, the Compensation Committee of the Board of Directors of the Company determines performance against the applicable performance-based conditions and/or market conditions. Generally, PSUs vest upon
the determination by the Compensation Committee of the Board of Directors of the Company of the achievement of applicable performance-based conditions and/or market conditions,, unless subject to earlier vesting, such as upon a Termination without Cause (as defined in the Plan) following a Change-in-Control of the Company (as defined in the Plan). PSUs do not convey voting rights.
The following table summarizes the PSU activity under the Plan:
| | | | | | | | | | | |
| Number of Shares | | Grant Date Fair Value |
| Unvested and outstanding at January 1, 2023 | — | | | $ | — | |
Granted | 781,132 | | | 31.91 | |
| Vested | — | | | — | |
| Forfeited | (5,103) | | | 27.61 | |
| Unvested and outstanding at December 31, 2023 | 776,029 | | | $ | 31.94 | |
Granted | 904,960 | | | 22.92 | |
| Vested | (15,735) | | | 29.93 | |
| Forfeited | (27,573) | | | 29.05 | |
| Unvested and outstanding at December 31, 2024 | 1,637,681 | | | $ | 27.02 | |
Granted | 826,270 | | | 25.21 | |
| Vested | — | | | — | |
| Forfeited | (20,620) | | | 27.07 | |
| Unvested and outstanding at December 31, 2025 | 2,443,331 | | | $ | 26.41 | |
|
|
Stock-based compensation expense
Total stock-based compensation expense was approximately $71.1 million, $56.7 million and $37.1 million for the years ended December 31, 2025, 2024, and 2023 respectively. At December 31, 2025, there was approximately $86.2 million of unrecognized stock-based compensation expense related to unvested awards that is expected to be recognized over a weighted-average period of 1.0 year. As of December 31, 2025, the total intrinsic value of options exercised and the total fair value of shares vested for the 2025 period was approximately $15.3 million and $7.6 million, respectively.
Stock-based compensation expense was classified in the consolidated statements of operations as follows:
| | | | | | | | | | | | | | | | | |
| For the Years Ended December 31, |
| (Dollars in Thousands) | 2025 | | 2024 | | 2023 |
| Cost of platform | $ | 25,391 | | | $ | 18,781 | | | $ | 11,980 | |
| Sales and marketing | 5,416 | | | 4,097 | | | 2,475 | |
| General and administrative | 40,261 | | | 33,802 | | | 22,643 | |
| Total stock-based compensation | $ | 71,068 | | | $ | 56,680 | | | $ | 37,098 | |
12. Employee Benefit Plans
The Company has an elective 401(k) savings plan that provides a 3.0% safe harbor contribution to all employees. In addition, a minimum profit-sharing contribution is required to satisfy year end plan testing. The profit-sharing contribution was approximately 1.5% in 2025 and 2024, and 1.4% in 2023. The Company made contributions of approximately $6.0 million, $5.6 million and $4.7 million for the years ended December 31, 2025, 2024, and 2023, respectively, recorded within Cost of platform, Sales and marketing and General and administrative expense within the accompanying consolidated statements of operations.
13. Commitments and Contingencies
There are no material commitments and contingencies as of December 31, 2025, or 2024.
We are currently involved in, and may in the future become involved in, legal proceedings, claims and investigations in the ordinary course of our business, including medical malpractice claims. These claims or proceedings can involve various types of parties, including governments, competitors, customers, partners, suppliers, service providers, licensees, licensors, employees, or stockholders, among others. When management determines that a loss is both probable and reasonably estimable, we accrue for loss contingencies associated with outstanding litigation. Although the results of these legal proceedings, claims and investigations cannot be predicted with certainty, we do not believe that the final outcome of any matters that we are currently involved in are reasonably likely to have a material adverse effect on our business, financial condition or results of operations. Regardless of final outcomes, however, any such proceedings, claims, and investigations may nonetheless impose a significant burden on management and employees and be costly to defend, with unfavorable preliminary or interim rulings.
14. Concentrations of Credit Risk
Our financial instruments that are potentially subject to concentrations of credit risk consist primarily of cash, cash equivalents, and accounts receivable. While the Company’s cash and cash equivalents are managed by reputable financial institutions, the Company’s cash balances with the individual institutions may at times exceed the federally insured limits. At December 31, 2025, substantially all of the Company’s cash and cash equivalents were held at two major financial institutions.
The following table provides the Company’s revenue concentrations with respect to payers comprising 10% or more of the Company’s total revenues (n/a - indicates balance or activity that is less than 10%):
| | | | | | | | | | | | | | | | | |
| For the Years Ended December 31, |
| (Dollars in Thousands) | 2025 | | 2024 | | 2023 |
| Payer A | 28 | % | | 26 | % | | 23 | % |
| Payer B | 18 | % | | 17 | % | | 16 | % |
| Payer C | 16 | % | | 15 | % | | 15 | % |
| Payer D | n/a | | n/a | | 10 | % |
The following table provides the Company’s concentrations of credit risk with respect to payers comprising 10% or more of the Company’s receivables, net (n/a - indicates balance or activity that is less than 10%):
| | | | | | | | | | | | | |
| For the Years Ended December 31, |
| (Dollars in Thousands) | 2025 | | 2024 | | |
| Payer A | 43 | % | | 46 | % | | |
| Payer B | 19 | % | | 19 | % | | |
| Payer C | 12 | % | | 14 | % | | |
| | | | | |
| | | | | |
| | | | | |
15. Net Income Per Share
A reconciliation of net income available to common stockholders and the number of shares in the calculation of basic and diluted earnings income per share was calculated as follows:
| | | | | | | | | | | | | | | | | |
| For the Years Ended December 31, |
| (in thousands, except for share and per share amounts) | 2025 | | 2024 | | 2023 |
Net income attributable to Privia Health Group, Inc. common stockholders | $ | 22,919 | | | $ | 14,385 | | | $ | 23,079 | |
| Weighted average common shares outstanding - basic | 122,176,587 | | | 119,402,749 | | | 116,731,406 | |
| | | | | |
| Weighted average common share outstanding - diluted | 128,889,836 | | | 125,614,171 | | | 124,686,067 | |
Earnings per share attributable to Privia Health Group, Inc. common stockholders – basic | $ | 0.19 | | | $ | 0.12 | | | $ | 0.20 | |
Earnings per share attributable to Privia Health Group, Inc. common stockholders – diluted | $ | 0.18 | | | $ | 0.11 | | | $ | 0.19 | |
Below are the weighted-average diluted shares outstanding that were excluded from the computation of diluted loss per share attributable to common stockholders for the period presented because they were anti-dilutive:
| | | | | | | | | | | | | | | | | |
| For the Years Ended December 31, |
| 2025 | | 2024 | | 2023 |
| Weighted-average antidilutive shares outstanding | 2,717,690 | | | 6,614,649 | | | 3,648,907 | |
16. Segment Financial Information
Management determined in accordance with ASC Topic 280, Segment Reporting (“ASC 280”), that the Company operates in and reports as a single operating segment, which is to care for its patients’ needs. Operating segments are identified as components of an enterprise where separate discrete financial information is available for evaluation by the CODM, or decision-making group, who reviews financial operating results on a regular basis for the purpose of allocating resources and evaluating financial performance.
The Company has concluded that its CODM is its Chief Executive Officer, who regularly reviews financial operating results on a consolidated basis for purposes of allocating resources and evaluating financial performance. Although the Company derives its revenues from a number of different geographic regions, the Company neither allocates resources based on the operating results from the individual regions, nor manages each individual region as a separate business unit. The Company’s CODM manages the Company’s operations on a consolidated basis and makes decisions regarding the allocation of corporate resources and the assessment
of overall consolidated profitability. As of December 31, 2025 and 2024, all of the Company’s long-lived assets were located in the United States.
The CODM uses consolidated net income attributable to Privia Health Group, Inc. to evaluate financial performance and allocate resources. Consolidated net income attributable to Privia Health Group, Inc. for the years ending December 31, 2025, 2024, and 2023 were $22.9 million, $14.4 million and $23.1 million, respectively.
F-31